Dear Members (a note from Deb Hickey):
I live in Massachusetts, about two hours north of Cape Cod, or “The Cape,” as we call it. In a couple of days, we’ll pack our Jeep Cherokee to the brim with bags, beach chairs, towels, coolers, and our six-year-old daughter and head to Harwich for the 4th of July. Of course, half the state, and many from out of state, will do the same. Route 3 South will become a parking lot filled with convertibles with rowdy teens, SUVs loaded with bike racks, and cars pulling campers.
For many, the 4th of July celebrations begin days before the fourth. It’s a festival of hot dogs, beach parties, parades, and fireworks. But what does “Independence Day” really mean? Do our children understand? Do we fully appreciate the significance of this holiday?
In July 1776, 56 brave men pledged their lives, their fortunes, and their sacred honor to secure our freedom. Because of these men and the actions that followed, we can enjoy today the liberties and promises that freedom brings. And on this holiday weekend, it includes simple things, like barbecues on the beach, displaying our flag, and watching parades.
It’s easy to get lost in the moment; to forget where it all began; to focus only on our summer plans and get swept up in the excitement of being with family and friends. But if those men hadn’t come forward and signed that parchment, our lives would be very different today.
When I think about my life and the family around me, I often think back to what brought us here—and I think of the people who have been a part of our present-day journey. Whether I know them personally or not—some played a very big role. My father, Bob Marckini, is 74-years-old. Nearly 17 years ago, I thought he was going to die from prostate cancer. Or if not, I worried that the quality of his life would be significantly and forever altered. Neither of those things happened and, for that I am grateful.
This year, we’ve decided to do things a bit differently. After visiting friends on the Cape for the holiday, my family and I will drive north to Mattapoisett to be with my parents for a couple of days before going home to Medfield. We’ll spend time at their beach, hunting for crabs with a plastic shovel and fishing for minnows with my daughter’s pink net. Every summer, my father spends hours in the tidal pools at the beach with Gemma, and it’s her favorite thing to do—I mean, ever. I think she’d rather hunt crabs and minnows with Papa than eat an ice cream sundae. To me, it’s my favorite thing to watch.
Having my father here to spend these hours, hunched over rocks; his feet covered in seaweed, “fishing,” with my daughter is one of my greatest gifts. And I have Dr. James Slater, Dr. Jerry Slater, the gantry team and staff at Loma Linda University Cancer Center to thank for that gift.
Now, I’m not comparing the Slaters to America’s forefathers; I’m simply acknowledging and remembering the people who directly impacted my family and made our lives better. I think we all need to do a little more of that. This year, I’m making a point to teach my daughter about Independence Day, the American Flag, and what makes our country so special. We owe that to our children.
You may notice this issue of BOB Tales is a bit longer than usual; it’s a two-month issue. Our September newsletter will be distributed in late August. This month, we provide an update on the proposed critical Proton vs. IMRT study. We discuss the difference in side effects between intermittent and continuous hormonal therapy. And we include a special segment on dealing with a prostate cancer recurrence.
We hope you enjoy the July/August issue of BOB Tales. As always, we welcome your feedback—just send an email to [email protected].
Deb Hickey
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file.
In This Issue:
- Critical Proton vs. IMRT Study: PCORI Update
- Fewer Side Effects from Intermittent Hormonal Therapy vs. Continuous
- Special Segment: Dealing with a Recurrence
- Proton vs. IMRT: Question from a Member
- 2001: PSA 436: 16 Years Later: Happy 74th Birthday!
- Webinar: When Health Insurance Says No: Understanding Appeals
- BOB Member Donates 33 Gallons … of Blood!
.jpg)
Critical Proton vs. IMRT Study: PCORI Update
We reported in our May 2017 BOB Tales that a task force was formed to formulate a comprehensive study comparing proton therapy to IMRT for treating prostate cancer. The task force consists of representatives from most of the proton centers in the U.S. as well as many centers that practice IMRT. Also on the task force are representatives of proton-related equipment manufacturers as well as several patient stakeholders. Deb Hickey and Bob Marckini are among the patient stakeholders on the team. This gargantuan project and submittal process is being led by Dr. Nancy Mendenhall, medical director at University of Florida Health Proton Therapy Institute. The project is titled, A Prospective Comparative Study of Outcomes with Proton and Photon Radiation in Black and White Men.
The proposal is being presented to the Patient Centered Outcomes Research Institute (PCORI) in order to secure funding for this multi-institution, multi-year comprehensive study. Two prior submittals were rejected by PCORI. This is the third attempt (Third time’s a charm?).
 As reported in our June BOB Tales, the Letter of Intent was approved by PCORI and they invited the team to submit a formal, detailed proposal. Dr. Mendenhall worked night and day to finalize and submit the proposal by the May 17, 2017 deadline. She tells us that we will learn of their decision in November. Why it may take that long, we don’t know.
As reported in our June BOB Tales, the Letter of Intent was approved by PCORI and they invited the team to submit a formal, detailed proposal. Dr. Mendenhall worked night and day to finalize and submit the proposal by the May 17, 2017 deadline. She tells us that we will learn of their decision in November. Why it may take that long, we don’t know.
As we’ve said in the past, this is one of the most important initiatives under way in the proton world, as denials by private insurers to cover proton therapy are increasing. This is frustrating patients who are dealing with a cancer diagnosis and must battle their insurer for coverage.
We know that proton therapy deposits significantly less radiation to healthy tissue than IMRT. We know the laws of physics would predict that clinical outcomes should be superior when less radiation is delivered to healthy tissue. We know the likelihood of secondary cancers is much higher when higher levels of radiation are delivered to healthy tissue. And we know what several surveys of proton patients have reported in terms of disease-free survival and quality of life after treatment. Nevertheless, more and more private medical insurers have been refusing to cover (more expensive) proton therapy for prostate cancer because, they say, it has never been proven—through comprehensive prospective studies—to be superior to IMRT.
Sadly, as a result, many men have been faced with long and protracted battles with their insurers who have denied coverage. Some eventually win their appeals, but many do not. They are then faced with either paying out-of-pocket for proton therapy, or choosing a lower cost option that their medical insurer will cover.
This is our chance to set the record straight. Let’s hope and pray the PCORI submittal is approved. We can confidently predict what the outcome of such a study would be. Stay tuned.
Fewer Side Effects from Intermittent Hormonal Therapy vs. Continuous
The Journal of Urology (May 2017, Vol. 197, Issue 5, pp 1251-1257) noted that randomized trials have shown intermittent androgen deprivation therapy (ADT) for patients with advanced prostate cancer may improve sexual and physical functioning compared to continuous ADT, without compromising survival.
The Journal further reported on an important study involving almost 9,800 men over 65 years old with advanced prostate cancer. Outcomes examined included acute myocardial infarction, stroke, heart failure, Type 2 diabetes and fracture.
Conclusions from the study: “Intermittent ADT was associated with a lower risk of heart failure and fracture compared to continuous ADT. This raises toxicity concerns for continuous relative to intermittent therapy and suggests that intermittent ADT may represent a safer therapeutic choice in elderly men with advanced prostate cancer.”

Dealing with a Recurrence
By Bob Marckini
Over the past 17 years we have been asked many times why we don’t write about dealing with a recurrence of prostate cancer. Our answer has been: “We don’t write about prostate cancer recurrences because the number and percentage of prostate cancer recurrences after proton therapy are very small, so why focus on the negative? We prefer the BOB Tales to be an up-beat newsletter.”
Having said that, we have about 9,000 members in our group, and some have had to deal with rising PSA, which in some cases has led to a recurrence of their prostate cancer. We have also heard from some members who have asked us to write about this subject, even though they are not experiencing a recurrence.
Note: Recurrences can, and do happen with all treatment options. When I was in treatment in late 2000, about 5 percent of the patients being treated with protons at the Loma Linda University Cancer Center were former surgery patients who had chosen proton therapy for salvage treatment. And we routinely hear from patients who have had a recurrence after IMRT wondering if proton therapy could be used for salvage treatment.
Disclaimer
I am not a physician and cannot give medical advice. The information presented here is based on my own research as well as interactions with patients and doctors over the past 17 years. The following comments have not been reviewed by, nor have they been endorsed by any doctors or medical institutions.
Also, this is not intended to be a comprehensive, all-encompassing treatment of the subject. Instead, it is a summary overview of what patients have done in the past along with providing some information about emerging technologies that are giving patients more options when dealing with a recurrence. The information presented generally applies to recurrences following all types of radiotherapy, not just proton.
I will also attempt to report on, what I believe to be, the best practices we have observed from patients and the medical community in dealing with rising PSA and/or prostate cancer recurrence.
What is a Recurrence?
Some members contact us when they have a bump in their PSA months or years after treatment. Bumps—especially during the first couple of years after treatment—are common and are usually innocuous.
The system used by most radiation oncologists in the U.S. for determining biochemical recurrence of prostate cancer is referred to as the Phoenix definition. This states that biochemical failure is defined as an increase in PSA of 2 ng/mL or more above the nadir level. So, if your nadir (lowest) PSA level was 0.5, then biochemical failure would be defined as a PSA level of 2.5 or higher.
What is the Recurrence Rate for Proton Therapy?
There is no single or simple answer to this question. Why? Because the recurrence rate depends on pre-treatment cancer staging and the specific treatment received. Early stage prostate cancer enjoys the highest biochemical disease-free survival rate, well into the high 90 percent range at 10 years, while intermediate and aggressive prostate cancers have lower rates of disease-free survival during that same timeframe. Having said that, we have members of our group with very high pretreatment PSAs and with Gleason scores of 10 who are doing very well, 10 or more years after treatment. Fortunately, the overwhelming majority of our members are doing very well 10 or more years out.
Older-Technology Biopsy Techniques Contribute to the Problem
Part of the problem has to do with the older technology biopsy procedure and the accuracy of pre-treatment staging. The 30-year-old “blind biopsy,” which is still in common use can miss cancer in the prostate when it’s there, or it may find low-grade prostate cancer, and miss higher-grade lesions. This can have some impact on the success of any treatment chosen by the patient.
What if My PSA Rises after Treatment?
What is a patient to do if he has rising PSA and/or a prostate cancer recurrence?
The first thing to note is that PSA can rise for several reasons including the following:
- The prostate is stimulated from sexual activity, digital rectal exam, riding a bicycle, or something else.
- Prostate infection, such as prostatitis. Some men have chronic prostatitis.
- Laboratory error on the blood sample.
- Unexplained PSA “bumps” are common, especially during the first couple of years after treatment.
- Prostate cancer activity.
Based on these factors, one can conclude that a PSA bump, or even several increases in PSA, does not necessarily translate to a recurrence. It’s not uncommon for someone to have a PSA bump, only to find PSA to return to previous levels when retested.
What does a patient do if his PSA rises?
Depending on the circumstances, the first thing doctors typically recommend is to repeat the blood test. If PSA returns to previous levels, the problem is solved. If it was lab error, for example, you would know right away when your PSA returns to previous levels.
If the retest confirms higher PSA levels, doctors often put their patients on an antibiotic, such as Cipro, to help rule out a prostate infection. If PSA levels return to normal after the antibiotic, the problem is solved.
If PSA levels remain elevated or continue to rise, the more progressive doctors and medical institutions often prescribe advanced imaging techniques (such as 3-T multi-parametric MRI) to determine if there are any “hot spots” or lesions in, or around the prostate. If detected, they typically order a targeted biopsy to determine if the lesions are cancerous, and if so, the likelihood of aggressive cancer.
No ‘One-size-fits-all’ Solution
Not all recurrences are the same. Every recurrence is unique and typically requires a customized approach to deal with it.
In some cases, depending on PSA progression and the patient’s age, no treatment is necessary other than keeping track of PSA. A recurrence many years after radiotherapy often involves an indolent (slow-growing) cancer.
For more aggressive recurrent cancer, doctors can order new, state-of-the-art imaging, such as the C-11 Choline PET/CT scan, the C-11 Acetate PET/CT scan, or the Blue Earth Diagnostics Axumin scan, which are available at selected locations around the country. These tests are capable of finding tiny lesions and detecting only living cancer cells. Tests like these help to identify “hot spots” anywhere in the body. Depending on the location and number of hot spots (lesions), specific treatment options can be prescribed.
Treatments for localized recurrences can range from oral medications, cryotherapy, High Intensity Focused Ultrasound (HIFU), brachytherapy (radioactive seeds), salvage radical prostatectomy, or other localized treatment modalities such as stereotactic beam radiation treatment (SBRT).
What about Metastasis?
Metastasis refers to cancer moving to locations distant from the original cancer site. Oligometastatic disease refers to a small number of lesions distant from the original tumor. Many doctors are dealing with oligometastatic disease with curative intent, often using focal treatment techniques.
Treatment for metastatic disease can range from androgen depravation therapy (hormonal therapy, such as Lupron), chemotherapy (many forms), immunotherapy or some combination of these.
In addition to these, there are new, emerging therapies for dealing with advanced, metastatic prostate cancer, such as vaccines and genetically modified viruses that manipulate blood cells from the patient’s immune system causing them to attack the prostate cancer. As pointed out in our discussion of the anti-cancer lifestyle in earlier issues of BOB Tales, there are a number of additional supportive strategies available to help combat cancer cells, including use of anti-inflammatory agents and lifestyle strategies intended to reduce stress.
Summary
A cancer recurrence can happen with all types of prostate cancer treatment options: surgery, conventional radiation, proton beam therapy, brachytherapy, cryotherapy, HIFU, etc. Our focus here has been recurrences after radiotherapy (proton or conventional radiation). PSA bumps are common and are usually meaningless. Rising PSA may be a result of several benign causes, or possibly a return of prostate cancer. Even if prostate cancer returns, it may not need any treatment depending on the aggressiveness of the cancer and the patient’s age. If treatment is needed, there are new imaging technologies that help determine the location, size and often the aggressiveness of the lesion(s). There are a large number of treatment options available for early-, moderate- and advanced-stage recurrences. And newer treatment options under development are showing great promise.
As always, your doctor is the first place to start if a recurrence is suspected. And getting second and third opinions is always recommended, especially from one of the preeminent cancer treatment centers.
Our intent with this piece is to give you information you can use in discussions with your doctor if you are ever faced with rising PSA or a recurrence. As stated above, thankfully for the overwhelming majority of us, our primary treatment worked and left us cancer free.

Recap: Pacific Northwest BOB Reunion
The 10th annual Pacific Northwest BOB reunion was held May 25, 2017 at the Portland Adventist Medical Center. There were 36 attendees including former proton patients, prospective proton patients and family members. The group shared their personal experiences while enjoying a buffet dinner. LLUCC staff members updated the group on Loma Linda’s Vision 2020 and also discussed planned giving opportunities. At the end of the evening, everyone watched a short video of Dr. Lynn Martell who welcomed and thanked them for attending.


Proton vs. IMRT: Question from a Member
A Canadian BOB member emailed Bob Marckini last month with a question we are frequently asked in various contexts. Below is the question and Bob’s answer. This information may be helpful to members who are asked similar questions by friends and acquaintances.
Question:
A prostate cancer site-administrator who—let’s say has never been pro-proton—recently responded to a question from a Canadian patient on proton vs. IMRT as follows:
The two things that I would say about proton beam radiation therapy (PBRT) are these:
- While it’s certainly true that PBRT is safer and comes with fewer side-effects than the old-fashioned, 3D conformal radiation therapy, to which it was originally compared, no one has ever shown in an appropriate clinical trial (or even in a large meta-analysis of data from small trials) that it is significantly safer or more effective than modern forms of high-quality, image-guided, intensity-modulated radiation therapy (IG/IMRT) that are customary at most specialized radiation therapy centers in the USA today.
- As a patient from Canada who would probably be paying for this form of treatment himself in the U.S., the cost of PBRT is liable to be extremely high. In the USA most of the major insurance providers have simply stopped paying for PBRT because they consider the cost too high when compared to the quality of the outcomes.
So, while I would never discourage a patient like you from investigating whether PBRT might be the most appropriate form of treatment, you do need to be aware of these two issues up front.
Bob, does he have his facts right? —Bill W.
Bob's Response:
Yes and no, Bill.
Practitioners and proponents of IMRT often use these arguments, out of context, to prevent proton from infringing on their “business.” Here are a few facts:
All radiation oncologists agree (both IMRT practitioners and proton) that the only safe dose of radiation to healthy tissue is a zero dose, and proton comes closer to that goal than any other form of radiotherapy. Most radiation oncologists also agree that proton therapy is the best choice when treating pediatric patients for two reasons: 1) proton does a much better job at targeting the tumor while sparing healthy tissue around the tumor. This saves the child from lifelong issues, including stunted growth of any limb in the region of treatment, and 2) the probability of secondary cancer later in life is markedly higher with IMRT than with proton.
If this is true, then why isn’t proton superior to IMRT when treating a man’s prostate? Think about all the important parts of the male anatomy surrounding the prostate (rectum, bladder, testicles, etc.). These too are spared, for the most part, when a prostate cancer patient is treated with protons. Also, secondary cancers can happen with men, especially younger men (50s and 60s) who are treated with radiotherapy. If the probability is lower for children when treating with protons, then why wouldn’t it also be lower when treating men’s prostates with protons?
Regarding the fact that no prospective randomized clinical trials have been done to prove the superiority of proton over IMRT for treating prostate cancer, it’s not for lack of trying. Funding exists for just such a trial at MGH in Boston and UPenn in Philadelphia. The problem is that over the past several years, they have had great difficulty registering enough patients who would agree to be randomized once they learn the differences between IMRT and proton. So, that study is at a standstill.
Fortunately, as noted above, Dr. Nancy Mendenhall at Univ. of Florida has been working hard with a team of people representing a large number of proton treatment centers and IMRT centers in the U.S. (I’m one of several patient stakeholders on the team). They are attempting to secure funding from the Patient Centered Outcomes Research Institute to fund a prospective study comparing protons to IMRT for treating prostate cancer. Dr. Mendenhall has found a way around the “randomized patient” obstacle. The formal, comprehensive submittal was made last week. If approved, we will get the answers to the questions on the table. It will take time, however, to sign up the 1,000+ patients and then a few years to reach the first significant data end-points. But it’s a start.
One last point: A recent article in MedPage Today quotes a Dr. Jatinder Palta, chairman of medical physics at Virginia Commonwealth University. When asked why more patients are not receiving proton therapy he replied, “One reason is that insurers are not covering most proton therapy.” But the other explanation is the disturbing one: Dr. Palta states, “Radiation oncologists don’t want to give away their income-producing patients. No provider is willing to give up patients, even though they know the long-term toxicity and morbidity of the patient they are treating with conventional therapy are bound to be higher.” Though this statement is quite revealing, we cannot assume all radiation oncologists think or behave this way. Nevertheless Dr. Palta’s observation is food for thought.
There is much more I could write on this subject, but I think this puts things in proper perspective.
2001: PSA 436, 2017: Happy 74th Birthday!
 BOB member Arnd Hallmeyer lives in Berlin, Germany. He is a physician in the field of occupational medicine. He was 57 when he was diagnosed with prostate cancer in 2001. His pretreatment PSA reading was 436 (!). Arnd became “deeply depressed,” thinking he was probably going to die. His father had died at the age of 58 from metastatic prostate cancer. In fact, for years, Arnd had avoided visits to his urologist. During his early professional career, Arnd worked as a nurse and participated in prostatectomies of several patients. “I was afraid of ever being faced with prostate cancer and having to go through the same terrible experience of radical prostate surgery because I’ve seen the outcomes—impotence, castration, and wearing diapers for life … To me, it seemed better to die than to live a life after prostate surgery.”
BOB member Arnd Hallmeyer lives in Berlin, Germany. He is a physician in the field of occupational medicine. He was 57 when he was diagnosed with prostate cancer in 2001. His pretreatment PSA reading was 436 (!). Arnd became “deeply depressed,” thinking he was probably going to die. His father had died at the age of 58 from metastatic prostate cancer. In fact, for years, Arnd had avoided visits to his urologist. During his early professional career, Arnd worked as a nurse and participated in prostatectomies of several patients. “I was afraid of ever being faced with prostate cancer and having to go through the same terrible experience of radical prostate surgery because I’ve seen the outcomes—impotence, castration, and wearing diapers for life … To me, it seemed better to die than to live a life after prostate surgery.”
The only reason Arnd finally went to his urologist was due to heavy bone pain. His wife, also a physician, urged him to go. After his diagnosis, they searched for the best surgeon they could find. Arnd remembers asking a well-known radiologist for recommendations and his answer was, “You don’t need a surgeon. You need Loma Linda.”
In December 2000, Arnd traveled from Berlin to Loma Linda University Cancer Center for the first time. He began proton treatment in January 2001. Arnd received proton therapy, and—because of his extremely high PSA—photon treatment as well. He also received hormone blockers.
Although Arnd’s English was limited at the time, he settled in and made friends easily. “The staff and Loma Linda soon felt like family,” he said. He scheduled his treatments for early in the morning or late in the afternoon so that he could hike in the mountains of the San Bernardino valley. “Coming closer to heaven, I found a better way back to earth,” he said of his experience.
Last month, Arnd celebrated his 74th birthday. He’s doing well and his PSA has been close to zero for many years. “I found the road again, and have realized that the best place for healing remains Loma Linda, CA.” Arnd still refers patients to LLUCC and has repeatedly witnessed “the transformation of devastated cancer patients to thriving survivors.” Happy birthday, Arnd!
Dog Notes: We Knew This Would Happen
In last month’s opening memo, Bob Marckini wrote about his beloved Bichon Frise, Sadie, for June’s “Bring Your Dog to Work Day” holiday. We asked members who have special dogs in their lives to write in and tell us about them. We were inundated with emails. We chose just a handful to include due to lack of space; they are below. Enjoy!
Pat Greany and Mitzi (Tallahassee, FL)
 I enjoyed the introductory remarks and photo re: Sadie! My almost 12-year-old poodle, Mitzi, and I are also constant companions. She sleeps on a bed under my desk while I’m working. She goes everywhere with me (Home Depot, Lowes, etc.) and brings joy and happiness to many people every time we go out. When folks see her, they can’t wait to pet her and from the look on their faces, I know they’re getting an endorphin rush! She’s also my personal therapy dog and best friend.
I enjoyed the introductory remarks and photo re: Sadie! My almost 12-year-old poodle, Mitzi, and I are also constant companions. She sleeps on a bed under my desk while I’m working. She goes everywhere with me (Home Depot, Lowes, etc.) and brings joy and happiness to many people every time we go out. When folks see her, they can’t wait to pet her and from the look on their faces, I know they’re getting an endorphin rush! She’s also my personal therapy dog and best friend.
Chuck Bloodgood and Big Mack (Salmon, ID)
We had a Makenzie River Husky named “Big Mack.” He was bred for the Makenzie River miners. The Forest Service wouldn’t let the miners build a road to their mines, so these dogs were bred to haul the ore from the mine on a metal sled. He was a very gentle dog and the kids either rode him or let him pull them around on a sled or wagon. He weighed in at 130 pounds. We had Mack for about 10 years and he is now buried under our apple tree, wrapped in one of our grandson’s blankets who insisted that we put the blanket around him before we buried him.
Always love your dog … They will always love you.
Glen Fotre and Molly (Prescott Valley, AZ)
 Molly was my “caregiver” during my treatment at LLUCC in 2011. She is a 13-year-old Havanese whom we adopted at the Yavapai County Humane Society when she was 6 (however it’s more like she adopted me—and she insisted on coming to Loma Linda with me). Havanese is the national dog of Cuba and was admitted to AKC in 1996. They are the result of puppies that the Spanish traders brought to Cuba during the 1800s as gifts to the Cuban traders’ wives. During the Communist takeover of Havana, most of the aristocracy moved to Miami and brought their dogs with them. At last count, there were about 4,500 registered with AKC. They are indeed related to the Bichon Frise!
Molly was my “caregiver” during my treatment at LLUCC in 2011. She is a 13-year-old Havanese whom we adopted at the Yavapai County Humane Society when she was 6 (however it’s more like she adopted me—and she insisted on coming to Loma Linda with me). Havanese is the national dog of Cuba and was admitted to AKC in 1996. They are the result of puppies that the Spanish traders brought to Cuba during the 1800s as gifts to the Cuban traders’ wives. During the Communist takeover of Havana, most of the aristocracy moved to Miami and brought their dogs with them. At last count, there were about 4,500 registered with AKC. They are indeed related to the Bichon Frise!
Insurance Issues: Legal Counsel Needed
Did you hire an attorney to help overturn a medical insurance denial for your proton treatment? If so, please let us know a) if you found your attorney to be knowledgeable about proton therapy and medical insurance denials in general, and b) if you were successful in overturning a denial.
As many private insurers are denying coverage for proton therapy for prostate cancer patients, we routinely hear from prospective patients who are attempting to be treated at proton centers in the U.S. that have been told their provider will not cover treatment and/or they have received a denial. Although we encourage them to contact the proton center for assistance, as many have dedicated staff hired solely to help with insurance issues, legal counsel is sometimes needed.
We have a short list of attorneys who have helped a BOB member/proton patient with insurance issues, but the list is several years old and we suspect there are more attorneys out there who have experience or would be willing to help patients obtain coverage for proton therapy.
If you have any legal contacts or have used an attorney who has been successful in assisting you, or someone you know, with an appeal, please send us their names and contact information. Thank you!
 Webinar: When Health Insurance Says No: Understanding Appeals
Webinar: When Health Insurance Says No: Understanding Appeals
Unfortunately, many of our members have had issues obtaining health insurance coverage for their proton therapy, especially in the past few years. Many have received denials and worked hard to overturn them; some have paid out of pocket. Many of you are still fighting your health insurance providers.
On Wednesday, August 16, Triage Cancer is holding a free webinar, When Health Insurance Says No: Understanding Appeals, that we think may be of interest to some of our members. The presentation will describe the appeals process for private health insurance, employer-sponsored health insurance, Medicare, and Medicaid. The webinar begins at 1:00pm PST/3:00pm CST/4:00pm EST. Register here.
 Another Member Pens Book
Another Member Pens Book
BOB Member Dick Tomassini was treated for his prostate cancer with proton therapy at Mass General Hospital in 2012. After his treatment, he wrote and published a book about his experience. Train Track Stories: The Holy Spirit, Lost Sheep, and Cancer is Dick’s personal account of battling prostate cancer and how the grace of God enabled him to get his mind off the disease and minister to people in need while traveling by train to a Boston hospital every day—people he met on the train, in the streets, and even in the hospital.
When Dick received the dreaded diagnosis, he explains, “It was like being manipulated by a judo throw—suddenly you find yourself off-balance, about to be tossed through the air, and you are not sure how to break the fall.”
Before Dick decided to undergo proton therapy, he was scheduled for surgery. At the same time, he sorted through various treatment modalities, which he refers to as “confusing and technical,” causing him much disappointment and uncertainty. Shortly thereafter, he spoke with a priest and found his way to proton therapy.
Feedback from New Member
New BOB member John Stark wrote an email to Deb upon his recent proton “graduation” at Loma Linda University Cancer Center:
They treated the “whole man” as I feel better informed about my health and how to live the rest of my life. It started the day I arrived.

A BOB Member’s Story: Why I Give Back
Written by BOB member Bob Hawley
I was getting annual PSAs, but missed a year. When I got my next PSA (age 60), it was elevated slightly, but still considered normal in 2006. However, my annual exam revealed hematuria, so the usual tests were done: IVP, cystoscopy (I’d had kidney stones for years, so this was routine).
When the tests came back negative, my PCP referred me to a urologist. A DRE revealed hardness on one side of the prostate. He did a biopsy, which tested positive for prostate cancer—Gleason 7, T2a. He suggested surgery or radiation. When I mentioned protons (which I’d already decided on) he scowled and said he had a few patients who had protons, but he never heard from them again.
I later learned that a kidney stone too large to pass had caused the blood. I had a lithotripsy before I underwent proton therapy.
My father-in-law, a retired SdA pastor, had gone to Loma Linda University Cancer Center for proton treatment five years before (he’s also a member of the BOB). He recommended it highly, noting the lack of side-effects. So it was a slam dunk for me.
My proton treatment was wonderful, especially the camaraderie with the other patients and their spouses. My wife, Sherrill, and I were treated like royalty by the gantry teams and other personnel at LLUCC. We attended the Wednesday night meetings and the Tuesday “Lunch Bunch.” I had 44 proton treatments in the morning so we had the rest of the day to play.
I’ve felt fine since treatment and have recently started dieting and working out. I lost 20 pounds and my last PSA was 0.13.
I keep myself busy by volunteering for the Willamette Humane Society. I also donate blood at the Red Cross (every 56 days—I’m working on my 33rd gallon), and Sherrill and I are part of the Mt. Angel Community Emergency Response Team. CERT is a FEMA program designed to teach people to fill in the gap during a mass casualty/emergency when first responders are overwhelmed. I’m constantly taking classes to supplement my skills, such as Wilderness First Aid, Basic Life Support, how to take care of burn patients, and recently, I took a class on Tactical Emergency Casualty Care, which deals with active shooter incidents and mass trauma injuries. I’m also taking a class in mantracking, which teaches a scientific method of tracking people, such as those who get lost, Alzheimer’s patients who wander away, missing children, and others.
 For fun, I pilot my flying club’s Cherokee PA-28 140. I also enjoy gardening and reading. Sherrill and I also enjoy making soap the old-fashioned way. Recently I mailed a few of our favorites to Bob Marckini and Deb Hickey to thank them for all they do for us BOB members.
For fun, I pilot my flying club’s Cherokee PA-28 140. I also enjoy gardening and reading. Sherrill and I also enjoy making soap the old-fashioned way. Recently I mailed a few of our favorites to Bob Marckini and Deb Hickey to thank them for all they do for us BOB members.
You may have heard that I’m also a proof-reader for the BOB Tales newsletter. My reason for doing so may not be all that altruistic. Initially, I did it because Bob Marckini, whom I love and respect, asked me to after I edited his book. I love to edit and doing it for such a great cause—proton therapy, the BOB, and all its members—makes it that much more important. Thanks to all the effort put into the BOB Tales newsletter! I think it’s one of the best publications out there.
I also started donating annually to the Robert Marckini Chair for proton research at LLUCC when I began selling BOB bumper stickers. The stickers read “Prostate Cancer? www.protonbob.com.” Occasionally, an “ad” is included in the BOB Tales newsletter urging folks to buy one, but it hasn’t raised much. They are $6.00 and proceeds go to the Marckini Chair.
 Traffic Alert
Traffic Alert
Build awareness about proton therapy on the road with a BOB bumper sticker. Send $6.00 to Bob Hawley: P.O. Box 45, Mt. Angel, OR 97362 and he’ll mail you one. Questions? Email Bob at [email protected].
I donate a set amount to proton research at LLUCC each year, no matter how many bumper stickers sell. It’s not a large amount, but it’s something I can do to help the awesome cause that saved my life and preserved the quality of my life. The more we can do to promote this wonderful treatment, the more it will become accepted, even commonplace and routine. Perhaps, more healthcare providers will be willing to pay for proton treatment some day (unlike Kaiser, which refused to pay for mine). Thanks to the Veterans Administration, which considered my prostate cancer the result of exposure to Agent Orange in Vietnam, I received 100 percent disability from the date I was diagnosed until well after treatment ended. I was able to repay the money my mother gave me for treatment.
BOB Comment
Seems to us, Bob is an all-around, extremely giving person—after all these years of knowing him, we were not surprised to learn about all of the volunteer activities he is involved in!
Bob, we are truly thankful for all that you do. And we know without your professional editing and thorough review of our newsletter, we’d have a lot more grammatical errors and typos! Thank you.
 How to Contribute to Proton Research
How to Contribute to Proton Research
- Donate Online: Visit the LLUCC website. Make sure the “Designation Type” is set to “Proton” and the “Designation” is set to “Robert J. Marckini Chair."
- Send a Check: Make your check out to “LLUCC Proton” with “Marckini Chair” on the memo line and send to: LLUH, Office of Philanthropy, P.O. Box 2000, Loma Linda, CA 92354.
- Make a Call: Contribute by phone. Contact Elvia DeHaro at 909-558-5010
- Make a Future Gift: Contact Todd Mekelburg at the Office of Planned Giving at Loma Linda University Health at 909-558-5376 or [email protected].
- Other Ways to Give: Contact Matt Miller at the Office of Philanthropy at Loma Linda University Health at 909-558-3582 or [email protected].

When to Wash Your Hands
Everyone knows to wash their hands after using the bathroom and before eating, but according to the Center for Disease Control you should be washing your hands at other times as well:
- Before, during and after preparing or handling food
- After blowing your nose, coughing or sneezing
- After touching garbage
- After touching either an animal or animal food
Nuts to Disease
A review of 20 prospective studies led by researchers at Imperial College London and Harvard T.H. Chan School of Public Health showed that just a few nuts a day may significantly lower disease risk.
According to the studies, people who ate nuts had a 29 percent lower risk for coronary heart disease, 21 percent reduced risk for cardiovascular disease and 15 percent lower risk for cancer. Nut eaters also had a 52 percent lower risk for respiratory disease, 39 percent lower risk for diabetes and 75 percent reduced risk for infectious disease.
Most risk reduction for all diseases occurred in people who ate just one ounce of nuts per day—about two dozen almonds or 15 pecan halves.
Results of these studies were published in BMC Medicine.
Belly Fat is Worst for Well-being in Older Men
A recent study revealed a big belly had the biggest impact on men’s general health, and that as men’s waistlines grew, their quality of life and sense of well-being declined. Low testosterone, by comparison, had little effect on the men’s lives.
 Some of the health risks from obesity include high blood pressure, high LDL (bad) cholesterol, low HDL (good) cholesterol, heart disease, diabetes, stroke, and cancer. The study, which observed 598 men, ages 60-74, is a reminder that keeping your gut from growing is one of the most important things you can do as you get older.
Some of the health risks from obesity include high blood pressure, high LDL (bad) cholesterol, low HDL (good) cholesterol, heart disease, diabetes, stroke, and cancer. The study, which observed 598 men, ages 60-74, is a reminder that keeping your gut from growing is one of the most important things you can do as you get older.
Series: “Make Vegetables Taste Good”
This is the 11th segment on a subject that’s consistent with our Anticancer series that began in October 2016. We made it our mission to find recipes that make the most healthful vegetables (and other foods, in this case) taste delicious.
Loma Linda University Health has a series on their website called, “LIVE IT: In the Kitchen” that features short videos inspiring healthful, wholesome home cooking. In less than a minute, each episode demonstrates how to make quick-and-easy meals. Below each video, you’ll find the full recipe and cooking directions.
We recently tried another one of these recipes and according to Deb, the carrot soup “tastes like dessert.” Here are some health benefits of carrots followed by the recipe for creamy carrot soup.
- Lowers cholesterol
- Helps to improve vision
- Helps prevent heart attacks
- Reduces signs of premature aging
- Wards off certain cancers
- Boosts immune system
- Improves digestion
- Increases cardiovascular health
- Boosts oral health
- More
Creamy Carrot Soup
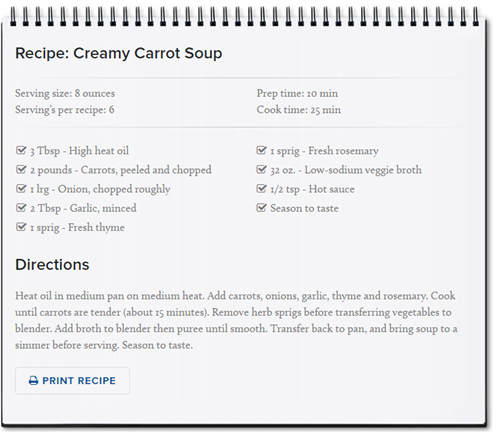
 Watch the video.
Watch the video.Want to share your healthful cooking tips and/or recipes with us? Send us an email.

How You Can Help Bob Marckini (and many others) in Just 1 Minute
Do you shop on Amazon? We’d be surprised if you didn’t; Amazon is widely considered the leader in ecommerce, perhaps the biggest ever seen in retail. What began about 20 years ago in a garage as an online bookstore has evolved into a retail giant—an amazon, if you will. Some researchers speculate Amazon has at least 66 million Prime (subscription) members. Not bad.
Why is Amazon so popular? For one, it brings together merchants and sellers from all over the world. Two, its product reviews have become uniquely famous in their own right—they are candid and plentiful. And studies show, they have an overwhelming effect on sales.
Finding Bob’s book after searching for “prostate cancer” on Amazon is still how most of our members first learn about proton treatment—in fact, take a look at the latest review below. Please keep the book front and center on Amazon. If you found it helpful in your journey to proton therapy and haven’t posted a review on Amazon, please do so today. Just click on the “Write a Review” button. It takes just a minute!
An excerpt from the most recent Amazon review:
 Bob’s decision to pursue proton therapy at Loma Linda University Medical Center is a MUST READ
Bob’s decision to pursue proton therapy at Loma Linda University Medical Center is a MUST READ
I came across Bob Marckini’s book on an Amazon search and I feel that I am now prepared to begin this journey. Bob has been exactly where I am today and his ability to tell a story of success in beating prostate cancer gives me TREMENDOUS hope … Bob’s book on his decision to pursue proton therapy at Loma Linda University Medical Center is a MUST READ if you or a loved one has been diagnosed with prostate cancer! —Tim H., 5/31/17
Buy Online, in Bulk or in Spanish
Online: Paperback: $19.00--•--Kindle: $9.99--•--NOOK Book: $9.99--•--Apple iBook: $9.99
In Bulk: Conctact us for a discount price list. Proceeds from book sales support proton therapy research through the Robert J. Marckini Endowed Chair at LLUCC.
In Spanish: Buy the print version or in eBook format.

Did You Know?
- In 1952, claims that smoking causes cancer caused Kent cigarettes to come out with an asbestos filter to protect its smokers!
- 1835 was the only time in U.S. history when the country was debt free, when Andrew Jackson paid off what he called “the national curse.” It lasted exactly one year.
- A tick bite can cause a lifetime allergy to red meat. The Lone Star tick injects a type of sugar found in red meat into the blood, resulting in antibodies that cause an allergic reaction when the person ingests meat.
- If you had invested $10,000 in Amazon stock when it went public 20 years ago, it would be worth $6,380,000 today—that’s almost 6.4 million dollars!
The United States Wins … Unfortunately
The obesity rate for Americans came in at an astounding 38.2 percent, which puts the U.S. at the top of the fattest nations-in-the-world rankings according to a survey from the Organization for Economic Cooperation and Development. Running second is Mexico at 32.4 percent of the population considered obese, followed by New Zealand, Hungary, and Australia. The UK comes in at number 6. In most countries, women are more obese than men.
The thinnest people come from Japan, with 3.7 percent obese, followed by India, Korea, Indonesia, and China. It’s not surprising that the cancer rates in these countries are so low.
And the future is fatter! The OECD reports that in the coming years, obesity rates are expected to increase, led by the U.S., Mexico and England, where 47 percent, 39 percent and 35 percent of the population are expected to be obese by 2030
Not All Thieves Are Stupid
GPS Theft
Someone had their car broken into while they were at a football game. Their car was parked on the green, which was adjacent to the football stadium, designated for fans. Things stolen from the car included a garage door remote control, some money, and a GPS which had been prominently mounted on the dashboard. When the victims got home, they found their house had been ransacked. The thieves had used the GPS to guide them to the house. They used the remote control to open the garage door and gain entry into the house. The thieves knew the owners were at the football game; they knew what time the game was scheduled to finish; and so they knew how much time they had to clean out the house. Something to consider if you have a GPS—don’t put your home address in it—put a nearby address (like a store or gas station) so you can still find your way home if you need to, but no one else will know where you live if your GPS is stolen.
Cell Phone
A lady has changed the way she lists names on her cell phone after her handbag was stolen. Her handbag, which contained her cell phone, credit card, wallet, etc., was stolen. Twenty minutes later when she called her husband from a pay phone telling him what had happened, he said, “I received your text asking about our pin number and I replied a little while ago.” When they rushed to the bank, they were told all their money was withdrawn. The thief had actually used the stolen cell phone to text the husband in the contact list to get the pin number. Within 20 minutes he had withdrawn all the money from their bank account.
Purse in the Grocery Cart Scam
 A lady went grocery shopping and left her purse sitting in the children’s seat of the cart while she reached for something on a shelf. During that time, her wallet was stolen and she reported it to the store personnel. Upon returning home, she received a phone call from the store’s security department. They told her they’d found her wallet and although there was no money in it, it still contained her personal papers. She immediately went to pick up her wallet, only to be told by security that they had not called her. By the time she returned home again, her house had been broken into and burglarized. The thieves knew that by calling and saying they were security, they could lure the woman out of her house long enough for them to burglarize it.
A lady went grocery shopping and left her purse sitting in the children’s seat of the cart while she reached for something on a shelf. During that time, her wallet was stolen and she reported it to the store personnel. Upon returning home, she received a phone call from the store’s security department. They told her they’d found her wallet and although there was no money in it, it still contained her personal papers. She immediately went to pick up her wallet, only to be told by security that they had not called her. By the time she returned home again, her house had been broken into and burglarized. The thieves knew that by calling and saying they were security, they could lure the woman out of her house long enough for them to burglarize it.

Last Month’s Brain Teaser
Say a painter can paint a garage in a day. His friend can paint a garage in two days. Working together, how long will it take for them to paint two garages?
Answer: 1 1/3 days. In that time the faster painter will have painted 1 + 1/3 garages, and his friend, who works half as fast, will have painted 2/3 of a garage, which totals two garages.
Here’s another way to look at it. Painter 1 paints a garage in 24 hours, or he paints 1/24 of a garage in one hour. Painter 2 paints a garage in 48 hours, so he paints 1/48 of a garage in one hour. Doing the math to find total hours: 2 garages ÷ (1/24 per hr + 1/48 per hr) = 2 ÷ 3/48 = 32 hours, which is 1 1/3 days
Winner: Several members got it right. The winner has not yet gotten back to us with permission to use his name. If we hear from him, we’ll write about him next month.
New Brain Teaser
If you’ve been a member for more than six years, you may have seen this one before.
Three closed boxes have all white marbles, all black marbles, or a mixture of both. They are labeled: “White,” “Black” and “Both.” However, you're told that each of the labels is wrong. You may reach into one of the boxes and pull out only one marble. Which box should you remove a marble from to determine the contents of all three boxes?
Send your answer to [email protected] for a chance to win a signed copy of Bob Marckini’s book, You Can Beat Prostate Cancer.
Bonus Trivia Question: What’s the most dangerous creature you are likely to encounter this summer? The surprising answer is at the end of the newsletter.
- A dog
- A bee
- A shark
- A rattlesnake
 ID ten T Error
ID ten T Error
Sometimes we older folks have trouble with computers. Yesterday, I had a problem, so I called Georgie, the 12-year-old next door (whose bedroom looks like Mission Control) and asked him to come over.
Georgie clicked a couple of buttons and solved the problem. As he was walking away, I called after him, “So, what was wrong?”
He replied, “It was an ID ten T error.”
I didn’t want to appear stupid, but nonetheless inquired, “An, ID ten T error? What’s that? In case I need to fix it again…”
Georgie grinned, “Haven’t you ever heard of an ID ten T error before?”
“No,” I replied.
“Write it down and I think you’ll figure it out,” he said.
So I wrote down: ID10T
That little brat.
The Cynical Philosopher
- I just read that 4,153,237 people got married last year. Not to cause any trouble, but shouldn’t that be an even number?
- I want to die peacefully in my sleep, like my grandfather. Not screaming and yelling like the passengers in his car.
- If I had a dollar for every girl that found me unattractive, they would eventually find me attractive.
- I find it ironic that the colors red, white, and blue stand for freedom until they are flashing behind you.
- A recent study found that women who carry a little extra weight live longer than the men who mention it.
- Money can’t buy happiness, but it keeps the kids in touch!
Power Failure
The power went out at my house this morning. My PC, laptop, TV, DVD, iPad, and my new surround-sound music system all shut down. Then I discovered that my mobile phone battery was dead, and to top it off, it was raining outside, so I couldn’t play golf.
I went into the kitchen to make coffee and then remembered the coffee pot also needs power, so I sat and talked with my wife for a couple of hours. She seems like a nice person.
Great Truths—2
“No man’s life, liberty, or property is safe while the legislature is in session.” —Mark Twain (1866)
“Talk is cheap, except when Congress does it.” —Anonymous
“The only difference between a tax man and a taxidermist is that the taxidermist leaves the skin.” —Mark Twain
“What this country needs are more unemployed politicians.” --Edward Langley, Artist (1928-1995)
“A government big enough to give you everything you want, is strong enough to take everything you have.” —Thomas Jefferson
What Not To Do Before a PSA Test
This is some important information for our members. Learn firsthand from professional racing cyclist Dan Atherton what not to do before a PSA test. Brace yourself and then watch the video.

Quote of the Month:
“Why do I have to swear on the Bible in court when the Ten Commandments cannot be displayed outside?”
— Unknown

Flashback from June 2015: A Simple Gesture
By John W. Schlatter, published in Chicken Soup for the Soul
One day, when I was a freshman in high school, I saw a kid from my class walking home from school. His name was Kyle. It looked like he was carrying all of his books. I thought to myself, “Why would anyone bring home all his books on a Friday? He must really be a nerd.”
I had quite a weekend planned (parties and a football game with my friends), so I shrugged my shoulders and went on. As I was walking, I saw a bunch of kids running toward him. They ran at him, knocking all his books out of his arms and tripping him so he landed in the dirt. His glasses went flying, and I saw them land in the grass about 10 feet from him. He looked up and I saw this terrible sadness in his eyes. My heart went out to him. So I jogged over to him, and as he crawled around looking for his glasses, I saw a tear in his eye. As I handed him his glasses, I said, “Those guys are jerks. They really should get lives.” He looked at me and said, “Thanks!” There was a big smile on his face. It was one of those smiles that showed real gratitude.
I helped him pick up his books, and asked him where he lived. As it turned out, he lived near me, so I asked him why I had never seen him before. He said he had gone to private school before. I would have never hung out with a private school kid before. We talked all the way home, and I carried some of his books. He turned out to be a pretty cool kid. I asked him if he wanted to play a little football with my friends. He said yes.
We hung out all weekend and the more I got to know Kyle, the more I liked him, and my friends thought the same of him. Monday morning came, and there was Kyle with the huge stack of books again. I stopped him and said, “Boy, you are gonna really build some serious muscles with this pile of books everyday!” He just laughed and handed me half the books.
Over the next four years, Kyle and I became best friends. When we were seniors, we began to think about college. Kyle decided on Georgetown, and I was going to Duke. I knew that we would always be friends, that the miles would never be a problem. He was going to be a doctor, and I was going for business on a football scholarship.
Kyle was valedictorian of our class. I teased him all the time about being a nerd. He had to prepare a speech for graduation. I was so glad it wasn’t me having to get up there and speak. Graduation day, I saw Kyle. He looked great. He was one of those guys that really found himself during high school. He filled out and actually looked good in glasses. He had more dates than I had and all the girls loved him. Boy, sometimes I was jealous. Today was one of those days. I could see that he was nervous about his speech. So, I smacked him on the back and said, “Hey, big guy, you’ll be great!” He looked at me with one of those looks (the really grateful one) and smiled. “Thanks,” he said.
As he started his speech, he cleared his throat, and began. “Graduation is a time to thank those who helped you make it through those tough years. Your parents, your teachers, your siblings, maybe a coach … but mostly your friends … I am here to tell all of you that being a friend to someone is the best gift you can give them. I am going to tell you a story.” I just looked at my friend with disbelief as he told the story of the first day we met.
He had planned to kill himself over the weekend. He talked of how he had cleaned out his locker so his Mom wouldn’t have to do it later and was carrying his stuff home. He looked hard at me and gave me a little smile. “Thankfully, I was saved. My friend saved me from doing the unspeakable.” I heard the gasp go through the crowd as this handsome, popular boy told us all about his weakest moment. I saw his mom and dad looking at me and smiling that same grateful smile. Not until that moment did I realize its depth.
Never underestimate the power of your actions. With one small gesture you can change a person’s life … for better or for worse. God puts us all in each other’s lives to impact one another in some way. Look for God in others.
Low PSAs to all,
Bob Marckini and Deb Hickey
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file.
Trivia Answer: In the average year, 43 Americans die from bee stings; 20 to 30 from dog bites, 5 to 10 from rattlesnake bites; and maybe one from a shark attack. If you have difficulty breathing or develop body hives after a bee sting, seek immediate medical attention.
NO MEDICAL ADVICE: Material appearing here represents opinions offered by non-medically-trained laypersons. Comments shown here should NEVER be interpreted as specific medical advice and must be used only as background information when consulting with a qualified medical professional.
Road Recognition
Build awareness about protons with a BOB bumper sticker. Just send $6.00 to Bob Hawley: P.O. Box 45, Mt. Angel, OR 97362 and he’ll mail you one. Or, email Bob at [email protected].
All proceeds go to the Robert J. Marckini Endowed Chair for proton therapy research at LLUCC.
Quote of the Month