By protonbob - March 30, 2022
Dear Members (a note from Bob Marckini):
Every once in a while, my daughter Deb “allows” me to write the opening memo for our monthly BOB Tales. I hope I can measure up to the new standard she’s set.
That Deb does an outstanding job with our monthly missives is clear because of the incredibly positive feedback we receive each month. Who would have guessed 21 years ago when we started publishing monthly newsletters, we’d still be doing this so many years later? And how they’ve improved – clearly because of Deb’s efforts!
Special Time with Deb
Speaking of Deb, I had a rare opportunity to spend some quality time with her last month. Deb’s been dealing with a rather rare and debilitating eye problem for the past couple of years. Meetings with the best eye specialists in the Greater Boston Area have not been able to resolve the issue, which is exacerbated by the hours she spends on the computer reading and responding to hundreds of emails as well as researching and writing our comprehensive newsletter.
A few months ago, one of the Boston physicians recommended Deb meet with a world-renowned neurologist who specializes in corneal neuropathy. The only appointment she could get was four months later at his Dover, NH office at 8:00 on a Friday morning in February. I volunteered to go with her, even though the drive from my home would be three to four hours from Cape Cod, through Boston traffic at rush hour. To complicate matters, a severe ice storm was forecasted. So, we decided to book rooms at a small motel in the seaside community of Portsmouth near the hospital and go up the night before.
I put four new, all-season tires on my SUV and picked up Deb at her home on Thursday evening. It was snowing heavily. The drive was an “event” to say the least. Traffic was awful; the roads were covered with snow and ice; and visibility was near zero. After a seemingly never-ending drive, we arrived safely, checked into our rooms, and went out to dinner at a local restaurant.
Notwithstanding the weather, the road conditions, and the reason for our visit, we had great conversation in the car, some laughs, a terrific dinner, and a restful night’s sleep. The next morning, the temperature had dropped to zero and I had to chip away an inch of ice just to open the car door. We made it to the appointment on time and had a productive meeting with the neurologist. Although there was no “aha moment” with the doctor, we felt Deb was in good hands. With his help and guidance, she should see some improvement in her symptoms.
Deb and I both look back on that trip to New Hampshire, our discussions in the car, and the dinner together as a pleasant interlude, a chance to spend some quality time together, discussing subjects other than prostate cancer, proton therapy, and backed-up emails. Despite the reason for the travel, it really was a fun time for both of us.
Last Month’s “Teaser”
This month’s BOB Tales is a special edition. Last month we “teased” you with a notice that we’d be telling you about one of the most important books on health, nutrition, and lifestyle we’ve come across. A few weeks ago, one of our long-time members and a dear friend called to tell me about a book he read that has changed his life. I dragged my feet in buying the book because I was backed-up with about six months of books and articles others have recommended or that I’d found on my own. So, I thought I’d work down that stack of reading material and then pick up the book he recommended. Fact is, I’m always reading articles and books on health, nutrition, and lifestyle in general, and on prostate cancer prevention, detection, and treatment in particular. These are subjects of particular interest to me. They also provide valuable information for our newsletters as well as future editions of my book.
In a more recent conversation with my friend, he brought up the book once again and urged me to read it. He convinced me, after he explained how the book has changed his life in so many ways, for the better. So, I bought the hard cover book as well as the audiobook, which is narrated by the author. And boy was he right! I mentioned my interest is in health, nutrition, lifestyle as well as prostate cancer prevention, detection, and treatment. Well, this book has all that, and much more. The book is titled, How Not to Die by Michael Greger, MD, with Gene Stone. Dr. Greger lists the top 15 causes of death and explains how the proper diet and lifestyle have the potential to prevent or reverse these diseases that are taking millions of lives each year.
In this month’s BOB Tales, our feature article in the Health section is the first in a series about this important book. I have little doubt that it will get your attention, and hopefully even influence you to make some changes in your lives. This month the focus is on prostate cancer. Next month we plan to cover the number one killer, heart disease.
Other Topics
Here are some additional topics we’ll be covering this month: Although it’s an uphill battle, we continue to see some important wins with patients challenging insurance company denials for proton therapy. The newer, safer transperineal prostate cancer biopsy is making news and is growing in popularity and use around the world. You’ll learn that maintaining proper body weight and healthy cholesterol levels can play an important role in preventing prostate cancer or a recurrence. There’s a terrific story about how one BOB member is “paying it forward.” And finally, we have an update on a critically important clinical trial, comparing proton therapy to IMRT, which Deb and I are deeply involved in.
As always, we love to get feedback on the newsletter, and welcome any suggestions you have on how to improve the value of the BOB Tales to our members.
Bob Marckini
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file. ![]()
![]()
In This Issue:
- Proton Therapy vs. IMRT for Prostate Cancer – COMPPARE Trial Update
- Court Finds Aetna Wrong for Denying Proton Therapy
- Transrectal vs. Transperineal Prostate Cancer Biopsy
- Treatment-related Regret Among Prostate Cancer Patients
- Overweight Men at Higher Risk of Recurring Prostate Cancer
- ‘How Not to Die’
- Magnesium May Prime Immune System to Fight Cancer

![]()
Proton Therapy vs. IMRT for Prostate Cancer — COMPPARE Trial Update
It’s been more than six months since we’ve provided an update on this critically important study comparing proton therapy to IMRT for prostate cancer, and we’re excited to let you know the latest. But first …
What does COMPPARE stand for?
COMPPARE stands for “A Prospective COMparative Study of Outcomes with Proton and Photon RAdiation in PRostate CancEr.” The COMPPARE trial will compare the quality of life, side effects, and cure rates for prostate cancer patients treated with proton therapy or photon therapy (IMRT).
Why is this study important?
 It’s the first of its kind – a multi-institutional, national trial that will directly compare the potential benefits and harms (cure rates and side effects) of protons versus photons (conventional X-ray radiation) in treating men with prostate cancer. It will emphasize patient-centered results and help future patients make informed treatment decisions.
It’s the first of its kind – a multi-institutional, national trial that will directly compare the potential benefits and harms (cure rates and side effects) of protons versus photons (conventional X-ray radiation) in treating men with prostate cancer. It will emphasize patient-centered results and help future patients make informed treatment decisions.
And, as you know, many health insurers refuse to cover proton therapy for prostate cancer due to its higher upfront cost and unanswered questions about its effectiveness compared to photon therapy.
The COMPPARE study should answer the question, once and for all, as to whether there are discernible differences between proton therapy and IMRT in treating prostate cancer.
Results of the study could resolve disagreements that are restricting patients’ access to proton therapy, particularly with regard to private medical insurers’ coverage and reimbursement policies.
Who’s leading the study?
The principal investigator is Nancy Mendenhall, MD, Professor, Dept. of Radiation Oncology and Medical Director, University of Florida Health Proton Therapy Institute (UFHPTI). The COMPPARE Consortium comprises a diverse group of clinicians, researchers, patients, and other stakeholders, all committed to directly comparing the potential benefits and harms of proton versus photon therapy.
Deb Hickey is one of 20 patient and caregiver stakeholders and Bob Marckini is one of eight on the executive board.
What’s the research team doing?
The COMPPARE research team is working with cancer clinics around the country – including 29 of the 40 U.S. proton therapy centers – to recruit men with localized prostate cancer, or cancer that hasn’t spread to other areas of the body. The trial will follow 3,000 prostate cancer patients who will be treated with either protons (1,500) or IMRT (1,500).
Who’s eligible?
To be eligible for the COMPPARE study you must be a man diagnosed with non-metastatic prostate cancer; a candidate for radiation therapy; and between the ages of 30-85 with a life expectancy more than eight years.
What’s new?
Bob and Deb planned to attend the annual COMPPARE workshop in Amelia Island, FL last month, however due to a surge in COVID-19 cases in the area, the event was canceled. It was instead held via Zoom.
Dr. Mendenhall and the team at UFHPTI did a superb job condensing the event into a one-day virtual conference. With comprehensive PowerPoint presentations and several guest speakers, attendees were informed of recent milestones achieved and newly established goals.
Proton Group Complete!
Hampton University Proton Therapy Institute recently enrolled the 2,000th COMPPARE participant and we’re two-thirds of the way through with accrual, an exceptional accomplishment given the ongoing challenges presented by COVID-19.
We’ve reached our goal of accruing 900 patients in the pragmatic proton therapy group – the cohort receiving the standard 44-treatment protocol – and we’re nearing completion of the randomized portion of the proton arm – those receiving the shortened treatment (hypofractionation) protocol. As for the IMRT group, which has been lagging behind proton enrollment all along, we hope to complete accrual sometime this fall.
An Interesting Reason for Lag in IMRT Recruitment
According to Dr. Mendenhall, a reason for the lag in IMRT accrual could be the increased use of ultra-hypofractionated radiation (also referred to as stereotactic body radiation therapy or SBRT). This involves higher doses of radiation over a much shorter period of time, typically five to seven treatments.
Results from two large trials comparing short- and long-course IMRT show no difference in outcomes. This is leading to wider acceptance of these shorter treatment regimens as standard-of-care when using conventional radiation.
When the COMPPARE trial was initially designed, there was no comparative effectiveness data for ultra-hypofractionation compared with conventional or moderately hypofractionated radiation with IMRT, nor was there any published data on the ultra-hypofractionation protocol with proton therapy. So, ultra-hypofractionation was not considered standard-of-care and therefore not permitted on the COMPPARE trial.
A recent survey of IMRT providers suggested that with recent data, along with COVID pressures, ultra-hypofractionation has been used more frequently and considered in most facilities as standard-of-care. After discussing this development with the COMPPARE study’s sponsors, research team, and scientific advisers, Dr. Mendenhall obtained approval to permit ultra-hypofractionation with IMRT on the trial (This does not pertain to the proton therapy cohort as enrollment is complete.)
Outreach to All Men
In the development of the COMPPARE team, Dr. Mendenhall established the Minority Engagement Group to develop local advocacy manpower for education, recruitment, enrollment, and dissemination of study results. Coordinated by Charles Griggs, engagement coordinator at UFHPTI, the group develops specific culturally appropriate educational materials and programs for use in local recruitment and works hard to ensure the COMPPARE trial represents all men.
We recently surpassed our goal of 10 percent black enrollment having accrued 14.8 percent. Although we’ve exceeded our goal, the team plans to continue to push the envelope on enrollment for black Americans.
Thank You and Congratulations!
The COMPPARE trial team has gone above and beyond to push this critically important study forward, working to gain approvals from the institutional review board, get sites registered and patients enrolled, launch and maintain a comprehensive newsletter, educate its stakeholders and find and take part in relevant outreach activities.
Bob and Deb are honored and excited to be a part of this effort, and believe it will mean big, positive changes for proton therapy – and thousands and thousands of cancer patients. Thank you and congratulations to the COMPPARE team for your tireless efforts to save lives and improve the quality of life for men being treated for prostate cancer.
If you have questions about the COMPPARE trial, visit the COMPPARE website and/or email [email protected].
Court Finds Aetna Wrong for Denying Proton Therapy
Written by Tim Rozelle, Associate Attorney, Kantor & Kantor, LLP & Founder, Proton Therapy Law Coalition
Judge Kenneth A. Marra in West Palm Beach, FL federal court recently issued a watershed decision in the ongoing fight in the courts to expand coverage and access to proton therapy. Issued January 27, 2022, Marra’s decision represents the first dispositive win in federal court for an individual’s or putative class member’s ERISA claims challenging insurers’ denials of proton therapy for various forms of cancer.
The decision is also a win specifically for one of the named plaintiffs, Mark Lemmerman, who was treated with proton therapy for prostate cancer.
Mr. Lemmerman was diagnosed with localized, non-metastatic prostate cancer in January 2020. His radiation oncologist recommended proton therapy as an alternative to IMRT to avoid delivering radiation to critical normal organs and tissues, including the bowel, bladder, and rectum.
The physician submitted a request to Aetna for proton therapy pre-authorization. Aetna referred the request to a third-party medical review vendor. After only an hour, the reviewer recommended Aetna deny the request on the ground that proton therapy was not medically necessary, citing an Aetna clinical bulletin.
Mr. Lemmerman’s physician appealed the decision. He included medical records and a letter outlining peer-reviewed medical literature and studies supporting his recommendation for proton treatment. Again, Aetna referred the appeal to a third-party medical review vendor and it was denied shortly thereafter.
Mr. Lemmerman then requested an external review, which Aetna referred to another third-party medical review vendor. The vendor upheld Aetna’s denial of coverage, stating that “the proposed treatment is considered experimental/investigational and not medically necessary per plan language for this individual under these unique circumstances.”
After having exhausted all levels of appeal, Mr. Lemmerman proceeded with his physician’s recommendation to undergo proton therapy and paid out-of-pocket. He also hired an attorney.
In analyzing the three denials, the reliance on Aetna’s clinical plan bulletin (CPB) in supporting those denials, and the lack of discretionary authority contained in the applicable plan documents at issue, the court held that Aetna’s decision to deny proton therapy coverage for Mr. Lemmerman was “de novo wrong, reflecting improper importation of CPB 270 criterion not found in the policy terms.” The court further held that Aetna erred in finding Mr. Lemmerman’s proton treatment not medically necessary.
The case will proceed to class action certification and trial.
Transrectal vs. Transperineal Prostate Cancer Biopsy
There is growing evidence that the new transperineal prostate biopsy system has distinct advantages over the older transrectal biopsy technique. We’ve reported on this subject in previous BOB Tales.
Badar Mian, MD, FACS, professor of surgery and urology at Albany Med Urology in Albany, NY recently recorded a video on this subject for Urology Times. In the video, Dr. Mian reports that infection rates are increasing with the (current standard) transrectal (TR) biopsy technique, which has been in practice for the past 30 years or more.
Dr. Mian suggests the increased infection rate may be connected with the overuse of antibiotics in the western world in recent years. “The thought [for transperineal (TP) biopsy] is that if you can avoid introducing some rectal bacteria into the tissue, that we may be able to totally avoid or at least minimize the post-biopsy infections,” he says. Note: Typically no antibiotics are needed for the TP biopsy.
Some urologists feel another possible advantage with the transperineal approach, is better cancer detection rates because the TP technique allows the doctor to sample parts of the prostate that have been somewhat inaccessible with the TR technique. But the primary advantage, Dr. Mian feels, is lower infection rates with the TP approach.
Treatment-related Regret Among Prostate Cancer Patients
Men with localized prostate cancer who undergo surgery are more likely to regret their decision than those who choose other treatment options, according to new research.
 Of 2,072 patients surveyed, 13 percent experienced treatment-related regret after five years, but treatment option varied among respondents. Sixteen percent (183) of prostatectomy patients regretted their decision; 11 percent (73) of radiotherapy patients, and 7 percent (20) of those who chose active surveillance. The main reason for remorse was that patients felt they weren’t fully informed of the risks and benefits of treatment and the risks of surgery, in particular.
Of 2,072 patients surveyed, 13 percent experienced treatment-related regret after five years, but treatment option varied among respondents. Sixteen percent (183) of prostatectomy patients regretted their decision; 11 percent (73) of radiotherapy patients, and 7 percent (20) of those who chose active surveillance. The main reason for remorse was that patients felt they weren’t fully informed of the risks and benefits of treatment and the risks of surgery, in particular.
This study is a good example of why it’s so important for men to educate themselves on each treatment option they’re considering, including active surveillance, and the pros and cons associated with each. Not surprisingly, regret was far more common among men who judged their treatment to be less effective than anticipated and side effects to be more severe.
The findings of this study suggest that more than one in 10 patients with localized prostate cancer experience treatment-related regret. The study’s authors recommended improved counseling at the time of diagnosis and before treatment, including a discussion and understanding of the patients’ values and priorities.
BOB Comment: It’s also important to consider that some doctors may tell you their treatment specialty is best, but they may not be knowledgeable about some of the other developing technologies. As Bob Marckini states in his second edition book, You Can Beat Prostate Cancer, it’s up to you, the patient, to do your homework and make the treatment decision that is best for you.
Note: We don’t believe the radiotherapy treatment option in this study included proton therapy.

We’ve been producing BOB Tales newsletters for more than 20 years. During this time there have been articles that many new members haven’t seen, and some older members may have forgotten. So, we periodically re-run articles from past newsletters. The following is from November 2006.
Overweight Men at Higher Risk of Recurring Prostate Cancer
Researchers evaluated data collected on 2,131 men who had undergone radical prostatectomy. In just under two years 12 percent of the men had their cancer return. There was a significant association between body mass index (BMI) and disease recurrence after factoring in the effect of ethnicity, age, and other conditions. Men with BMIs of 35 or greater were 69 percent more likely to have a recurrence of prostate cancer than men whose BMIs were 25 or less (normal weight). Men with BMIs greater than 30 had a 31 percent increased risk of recurrence than men with lower BMIs.
There are a number of potential mechanisms through which obesity could promote prostate recurrence, the researchers note. One mechanism could be from the effect of excess fat on hormone levels.
BMI weight status is as follows: Below 18.5 is considered underweight; 18.5-24.9 is normal weight; 25-29.9 is considered overweight; and 30.0+ is obese.
If you want to check your BMI, do an Internet search for “BMI calculator” and you’ll find lots of easy-to-use calculators; just enter your height and weight.
Healthy Cholesterol Levels Could Lower Prostate Cancer Risk (Associated Press)
Doctors have long known that lowering your cholesterol levels helps protect your heart. But could it also reduce the risk of prostate cancer for men? Researchers are increasingly optimistic that the two conditions are related, making what’s good for the heart good for the prostate, too.
A previous study by the National Prostate Cancer Coalition and Dr. Mark Moyad from the University of Michigan, demonstrated a link between high cholesterol levels and high rates of prostate cancer in African American men. Other studies have found men taking medications to reduce their cholesterol levels also reduced their risk of prostate cancer.

BOB Member Goes Above, Beyond and Back Again
Shortly after BOB member Vern Haase was diagnosed with prostate cancer in 2010, he took a camping trip to Arizona with friends. A few of them decided to get haircuts, so they visited a local barber shop. “As we sat there, a book in the waiting area caught my attention,” said Vern. It was the first edition of Bob Marckini’s book, You Can Beat Prostate Cancer. “I asked the owner if I could borrow it,” said Vern. “He told me I could keep it because one of his clients had given him 30 of them to hand out.”
After reading the book cover to cover, Vern’s decision was made. He was treated at Loma Linda University Cancer Center in late 2012, finishing up the day after Christmas. “When I got home, I gave a copy of Bob’s book to my urologist,” said Vern.
But that’s not all he did.
Talk About Paying it Forward!
Shortly after his proton treatment ended, Vern got together with a fellow “proton graduate” to start a local prostate cancer support group in his hometown of Omak, WA. Both decided that after having wonderful treatment experiences they wanted to “pay it forward” and help others. Vern’s wife Sandy helped too.
The purpose of the group was to educate men about proton therapy for prostate cancer through various means including information provided by LLUCC, articles gleaned from the BOB Tales newsletter, and tips from Bob Marckini’s book. Vern and several group members also worked hard to spread awareness about proton therapy for prostate cancer by doing the following:
- Posting announcements about their meetings in the community calendar section of local newspapers;
- Engaging with local newspapers to run stories about proton therapy;
- Writing letters to editors of various newspapers to promote proton therapy;
- Contacting radio stations to suggest/arrange programs about proton therapy;
- Creating posters and fliers about proton therapy to be displayed at doctors’ offices and exam rooms;
- Designing and printing thousands of “business cards” for members to hand out at their leisure;
- Buying and placing Bob Marckini’s books in medical clinics, pharmacies, barber shops, and other businesses within a 40-mile radius.
“We’ve also referred several men for proton treatment and not necessarily all prostate cancer patients,” said Vern. “In one case, a doctor told a man with bladder cancer he couldn’t treat him and to go home and get his affairs in order. I recommended he contact Loma Linda for a second opinion. Two years after proton treatment, he’s doing fine.”
10 Years Later
“We’re still going at it 10 years after my treatment ended,” said Vern. “We have anywhere between eight and 28 members join our meetings every month and some travel more than 125 miles to attend.” One of the groups newest members is a well-known dentist whose written two books on healthful eating and foods that fight cancer.
Vern still relies on the BOB Tales newsletter to inform and educate group members and others in his community.
“It’s my privilege to serve in this small way to help men find their way to proton therapy,” said Vern.

Don't Just Stand There
In an effort to boost funding for basic and clinical proton therapy research on prostate cancer, pancreatic cancer, liver cancer, breast cancer, and more, we asked our members to donate $100 (or more) to Loma Linda University Cancer Center. In return, they’d receive an advance copy of Dr. William Preston’s book, Don’t Just Stand There – Realizing a Vision for Proton Therapy: Conversations with James M. Slater, MD, FACR. The response so far has been phenomenal. Thank you to all who’ve requested a copy.
 If you’d like a pre-published copy of “Don’t Just Stand There,” please send a check for $100 or more, payable to “Loma Linda University Proton Cancer Research” and mail it to:
If you’d like a pre-published copy of “Don’t Just Stand There,” please send a check for $100 or more, payable to “Loma Linda University Proton Cancer Research” and mail it to:
Loma Linda University Health ● Office of Philanthropy ● PO Box 2000 ● Loma Linda, CA 92354
Please notify Deb Hickey at [email protected] that you’ve sent in your check and your book will be mailed immediately.
Don’t Just Stand There, which contains high-quality color images and illustrations, is not only about Dr. Slater’s quest to create the world’s first hospital-based proton treatment center. It's also a teaching guide. As the Proton Treatment & Research Center at Loma Linda was such an immense endeavor, Dr. Slater wondered if the aspects of conceiving, planning, and orchestrating such a project, among others he undertook, might be instructive to others. Over the years, he’d also met people in all walks of life, many of whom had dealt with large and complex problems. He was struck by some of the stories they told about their work. And although the fields or disciplines usually had nothing to do with medicine, many experiences were similar. And so, he kept this in mind while he worked on the book with Dr. Preston.
We’re sure you’ll thoroughly enjoy the book and we know it will occupy a place of honor
in your home. And, you’ll be helping to fund basic and clinical proton research on prostate cancer, pancreatic cancer, liver cancer, breast cancer, and much more with your tax-deductible gift. Thank you!
Giving Options
- Donate to proton research online.
- Write a check to LLUCC Proton (Put “Marckini Chair” on the memo line) and mail to LLUH, Office of Philanthropy P.O. Box 2000, Loma Linda, CA 92354.
- Make an unrestricted gift (put “unrestricted” on memo line) so LLUH can use it where it’s needed most.
- Call Regina Joseph at 909-558-5010 to donate over the phone.
.jpg)

“How Not to Die”
By Bob Marckini
While in treatment at Loma Linda more than 21 years ago, the patient support programs taught me a lot about the importance of reducing/eliminating red meats and animal fats from my diet, increasing my intake of fruits and vegetables, and maintaining a serious exercise regimen. I wasn’t surprised several years later, when the Seventh-day Adventist community at Loma Linda would be designated a “Blue Zone” by Dan Buettner, a National Geographic Fellow and bestselling author. Blue Zones refer to five places in the world where people are the healthiest and live the longest. These five places are Okinawa, Japan; Sardinia Italy; Nicoya, Costa Rica; Ikaria, Greece; and Loma Linda, CA. Not surprisingly, all five Blue Zones are not identical in all aspects of diet and lifestyle. However, they all share one common characteristic: they promote a diet rich in fruit, vegetables, whole grains, nuts and legumes (e.g., beans, peas, lentils).
My interest in this subject following treatment prompted me to read certain books, such as The China Study, by T. Colin Campbell; Anticancer a New Way of Life, by David Servan-Schreiber, M.D; Health Power: Health by Choice, Not by Chance, by Hans Diehl, MD, and Aileen Ludington, MD, and The Blue Zone, by Dan Buettner. These all added greatly to my knowledge and commitment to a healthier lifestyle. Many of the points made in these books have found their way into the latest edition of my book, in Chapter 10, Impact of Diet and Lifestyle on Prostate Cancer Prevention and Recurrence.
There’s another important book on this subject: How Not to Die, by Michael Greger, M.D.
It’s an unusual title for a book that could possibly change your life – in a good way. It was brought to my attention by a good friend and BOB member, Charles Smithgall. It certainly has changed his life. Since reading the book and changing his diet, Charles tells me he eats all he wants without gaining weight and his key vital signs have improved. For example, his bad (LDL) cholesterol is down; his good (HDL) cholesterol is up; and his total cholesterol is well below the upper limit. And, he says he feels so much better, by just about every measure. Charles called to tell me about this book with palpable excitement and enthusiasm. He convinced me to read it as well as listen to it on audiobook (it’s narrated by the author).
The author, Michael Greger, M.D., is founder of the popular, Nutritionfacts.org, a science-based nonprofit that provides updates on the latest in nutrition research. His book has 560 pages, which includes a 154-page appendix, with valuable information on supplements and an exhaustive bibliography with references on How Not to Die from the 15 leading causes of death.
At the beginning of this landmark book, Dr. Greger makes the point that most doctors are very good at treating acute illnesses, but they don’t do a good job of helping to prevent chronic diseases. He points out that the 15 leading causes of premature death take the lives of 1.6 million Americans annually, and this doesn’t have to happen. By reading Dr. Greger’s advice, which is backed-up by a mountain of documented scientific evidence, you can learn about diet and lifestyle choices that can help you slow, stop, and even reverse diseases to live a longer and happier life.
In addition to very specific diet and lifestyle recommendations for dealing with the top-15 causes of death, Dr. Greger’s book provides a list of “the daily dozen,” a checklist of foods and activities that he says we should incorporate into our daily routines.
What, then, are the 15 leading causes of death in the U.S.? They are heart disease, lung diseases, brain diseases, digestive cancers, infections, diabetes, high blood pressure, liver diseases, blood cancers, kidney disease, breast cancer, suicidal depression, prostate cancer, Parkinson’s Disease, and iatrogenic causes. This last one may surprise you – you may want to look it up.
Read Chapters in Any Order
After reading the brief introduction and preface, you can quickly skip to any chapter that interests you. In the coming months, we’ll explore a few of the diseases that Dr. Greger writes about, beginning with a subject our members might find of interest …
Chapter 13: How Not to Die from Prostate Cancer
In introducing this chapter, Dr. Greger relates the story of a man, Tony, who seemed to be doing everything right: He followed diet recommendations from the USDA; switched from whole milk to skim milk; from beef to fish and chicken; exercised regularly, including running; avoided tobacco, alcohol and drugs; maintained a healthy weight; and he even managed, somehow, to “choose” parents and grandparents who lived long, healthy lives.
In his early 50s, Tony was diagnosed with aggressive prostate cancer. He elected to have surgery at a world-renowned medical center, and it left him dealing with urinary incontinence and sexual dysfunction. It was after these events that Tony learned about Dr. Greger and his body of research. He has since followed Dr. Greger’s diet and lifestyle regimen and has had no recurrence of his cancer.
Are Dairy Products … and Chicken Bad for You?
 Dr. Greger points out that, “Humans are the only species who drink milk after weaning. It also seems a bit unnatural to drink the milk of another species.” But milk, often from genetically “improved” cows, contains sex steroid hormones, like estrogen. Even organic cow’s milk contains hormones that can impact the lives of people who drink it.
Dr. Greger points out that, “Humans are the only species who drink milk after weaning. It also seems a bit unnatural to drink the milk of another species.” But milk, often from genetically “improved” cows, contains sex steroid hormones, like estrogen. Even organic cow’s milk contains hormones that can impact the lives of people who drink it.
“Mother Nature designed cow’s milk to put a few hundred pounds on a baby calf within a few months,” Greger says. During a lifetime of consuming milk, it’s easy to see how these factors can be connected to certain cancers. The hormone amounts in milk could explain the five-fold increase in twin births vs. women who don’t drink milk. Greger also references studies that suggest dairy products could stimulate the growth of hormone-sensitive tumors and promote the conversion of precancerous lesions into invasive cancers.
Dr. Greger also reviewed other scientific studies and experiments that showed a dramatic increase in prostate cancer in Japanese men since WWII, coincidental with a significant increase in egg, meat and dairy consumption.
Other laboratory experiments showed that cow’s milk stimulated growth of prostate cancer in a petri dish, while, almond milk, for example, suppressed prostate cancer growth. Still other studies, documented in the book, showed that high intakes of dairy products like milk (including low-fat milk) and cheese appeared to increase prostate cancer risk. These findings did not show up with consumption of yogurt and soured milk, possibly due to the presence of bacteria in these foods.
A Harvard University study showed that men who consumed as little as a single egg a day appeared to have twice the risk of prostate cancer progression, including metastasis.
Poultry and Eggs
The Harvard study found that, even worse than eggs, was poultry. The same Harvard University study, according to Dr. Greger, reported that men “who regularly ate chicken and turkey had up to four times the risk of prostate cancer progression.” Researchers suggested this may be due to heterocyclic amines, which are cooked-meat carcinogens, that seem to be present in chicken and turkey meat, more so than in other animals.
Higher levels of choline, a nutrient that is present in some foods, has been associated with the risk of developing prostate cancer. A Harvard University paper titled, “Choline Intake and Risk of Lethal Prostate Cancer” reported that men who consume high levels of choline in foods, such as eggs, have a higher risk of dying from prostate cancer.
Patient Blood Experiment Shows Prostate Cancer Reversal
Dr. Greger reported on research done by Dr. Dean Ornish and Pritikin Research Foundation researchers, which showed that the blood of people who ate a plant-based diet was “dramatically less hospitable to cancer-cell growth than the blood of people in the control group who continued to eat their typical diet.”
A series of experiments showed that, while the blood of men on a standard American diet slowed the rate of prostate cancer progression by 9 percent, the blood of men on a plant-based diet suppressed cancer growth by 70 percent.
The combination of a plant-based diet plus exercise seemed to show the greatest benefit. In one study blood from volunteers was dripped onto prostate cancer cells growing in a petri dish. And not surprisingly, the blood from the control group with a standard American diet and minimal exercise killed about 1 to 2 percent of the cancer cells. A second group included individuals who exercised regularly. Blood from this group killed 2,000 percent more cancer cells than the control group. But the best results – 4,000 percent cancer cell destruction happened when using the blood from the group that exercised regularly and consumed a plant-based diet.
Dr. Greger went on to show that a healthful diet and lifestyle can not only help prevent prostate cancer, it also has the potential to treat or reverse other cancers as well as other medical conditions such as type-2 diabetes, hypertension, and heart disease.
Other Studies and Helpful Information
Another study involved men with early-stage prostate cancer who were doing active surveillance. They were split into two groups: one control group and another group that followed a strict plant-based diet plus an exercise regimen. After tracking all participants’ PSAs for a year, researchers observed the control group’s PSAs increasing an average of 6 percent, but the plant-based diet and exercise group saw their PSAs drop by an average of 4 percent, suggesting their tumors were shrinking. Other testing, including gene testing confirmed these findings.
Many more studies were done and are reported in this important chapter in Dr. Greger’s book. All point to the fact that a plant-based diet plus exercise can not only slow prostate cancer disease progression, i.e., slowing the increase in PSA, or PSA doubling time, it can often reverse the disease as indicated by a reversal in PSA progression.
Dr. Greger zeros in on what he considers to be the most important foods to avoid, which include eggs and poultry, as well as, perhaps the most important foods to add to your diet, which include cruciferous vegetables, such as broccoli, cauliflower, kale, cabbage and brussels sprouts.
He’s also a big fan of ground flaxseed which he says lowers cancer-cell proliferation rates. He reminds us to make sure it’s ground flaxseed, because unground flaxseed just passes through your body undigested.
Summary
Recent research has provided overwhelming evidence that diet and lifestyle are major factors in health promotion; cancer, autoimmune, and cardiovascular disease prevention; and even disease reversal. Multiple publications by highly credentialed authors presenting volumes of documented scientific evidence provide a convincing argument that certain foods are not only unhealthful, they can even promote the progression of certain diseases such as prostate cancer. Countless studies have shown that a whole food plant-based diet, especially when combined with an exercise regimen has been shown to be especially beneficial to overall health and appears to play a critically important role in slowing, stopping, and reversing prostate cancer and other diseases. As Dr. Michael Greger points out, “A prostate-healthy diet is a breast-healthy diet is a heart-healthy diet is a body-healthy diet.”
Next Month
Next month we’ll be reviewing Chapter 1 from Dr. Greger’s landmark book, How Not to Die, from our number 1 killer: heart disease.
Magnesium May Prime Immune System to Fight Cancer
Experts define magnesium as an “essential macromineral” or major mineral which means people need to consume it in relatively large amounts – at least 100 milligrams each day – in order to stay healthy. Magnesium-rich foods include nuts, legumes, whole grains, greens, and even dark chocolate.
Magnesium plays many crucial roles in the body. You need magnesium for muscle and nerve function, normal heart rhythm, blood sugar levels, to transport other minerals throughout the body, and for basic energy needs, according to the National Institutes of Health.
Promising Research Under Way
Research has found that cancer spreads more quickly in mice on a low-magnesium diet. The same animals also had weaker immune defenses against flu viruses. Although magnesium has been shown to support a healthy immune system, little research has been done to learn exactly how.
Scientists in Switzerland have discovered a type of immune cell – called a killer T cell – that can eliminate cancerous cells only in the presence of magnesium. They found that magnesium activates a protein on the surface of killer T cells and uses it to bind to the target cells. Researchers are looking at ways to boost the concentration of magnesium in the tumors of patients. They also plan to test whether giving magnesium supplements to cancer patients can improve results when given with two immune therapies. Clinical trials are ongoing.

 You Can Beat Prostate Cancer: And You Don’t Need Surgery to Do It –Second Edition
You Can Beat Prostate Cancer: And You Don’t Need Surgery to Do It –Second Edition
There are more than 130 reviews of Bob’s book on Amazon and it still sits in the No. 1 or No. 2 position out of more than 5,000 books on a search for “prostate cancer.” New reviews are being posted monthly, and almost all are five-star.
Following is a recent Amazon review:

Read this book before taking any action about prostate cancer: I read the first edition in 2012 when my PSA was 3.7. The urologist wanted to do a biopsy and I decided to wait. In June 2021 my PSA was 6.0. My regular doctor insisted I go back to the urologist. I bought the new edition of Bob Marckini’s book and read it. As a result, instead of a biopsy I asked the urologist for an MRI. He said my insurance probably would not pay for it. I asked him to order it and seek pre-approval and if denied I would appeal. The insurance approved it and the MRI was normal. So as a result of reading Bob’s book, I avoided a biopsy. In addition I have two friends who had biopsies and the urologist immediately said they needed to have the prostate removed. When they told me, I said “don’t do anything until you read this book,” and loaned them my book. Both men still have their prostates. Bob has done a wonderful service for men by writing this book.
Step 5 in the 10 Steps
In October we began excerpting from, perhaps, the most important chapter in Bob’s second edition book, Chapter 18, titled, “Ten Steps for Taking Control of the Detection and Treatment of Your Prostate Cancer.” Step 1 was “Choose Your Doctors Wisely;” Step 2, “Have a PSA Test and DRE as Part of Your Annual Physical, And Track the Results.” Step 3 was “Have a Multi-parametric MRI Imaging if PSA is Rising.” Step 4. Manage Your Biopsy Test if Above Steps Lead to a Decision to Schedule a Biopsy. Following are excerpts from Step 5:
Get a Second Opinion on Your Biopsy Results
I can’t overemphasize the importance of this step. When you finish reading this section, you’ll understand why I feel this way.
Gleason Score is Key
Your Gleason score is probably the most important factor in staging your cancer. It will have a major impact on whether you’re a candidate for active surveillance, as well as which of the treatment options might work for you.
Your Gleason score will also be a major influence on the need for any adjunct treatments, such as androgen deprivation (hormonal) therapy.
As you know from an earlier chapter the Gleason score is determined by a pathologist evaluating prostate tissue samples under a microscope and looking for five different cell patterns ranging from normal, well-differentiated cells all the way to significantly fused, amorphous cell patterns. He/she then takes the two most predominant patterns and adds them together, putting the most dominant cell-pattern first. This becomes your Gleason score.
While it may sound simple and straightforward, it’s not. The process is subjective at best, and errors are frequently made.
‘How Doctors Think’
Over the past several years, I’ve heard from dozens of men who’ve read my book and took my advice on seeking a second opinion on their biopsy slides, only to learn that the initial reading was incorrect.
How do we know the second reading is correct? If the second reading is done by one of the premier pathology labs at a highly respected medical center – such as Dr. Jonathan Epstein at Johns Hopkins – then you know it’s an accurate result that can be used for determining a treatment plan. I’ve provided a list of some of the premier pathology labs in the appendix.
I recently read the book, How Doctors Think, by Jerome Groopman, M.D., of Harvard Medical School. The book reviews Dr. Groopman’s experiences both as an oncologist and as a patient. If you ever doubt the importance of seeking a second opinion on medical matters – especially biopsy slides – read this book.
My assessment of the theme of his book is that doctors are human beings and human beings make mistakes. The patient should become his own advocate, do his research, challenge conclusions, and always ask questions. That is also the theme of this book.
Using radiology as an example, Dr. Groopman notes that in one study at Michigan State University radiologists disagreed among themselves 20 percent of the time! And the same radiologists contradict their earlier analyses 5 to 10 percent of the time.
In another study involving screening mammograms of 148 women, “the fraction of patients actually having cancer who were correctly diagnosed varied from 59 to 100 percent, and the fraction of patients without disease who were correctly diagnosed as normal ranged from 35 to 98 percent. Overall, the accuracy rate varied from 73 to 97 percent.”
Results from a variety of radiological procedures were summarized by Ehsan Samei of the Advanced Imaging Laboratories at Duke University Medical Center. He concluded that:
The average diagnostic error in interpreting medical images is in the 20 to 30 percent range. These errors, being either of the false-negative or false-positive type, have significant impact on patient care.
The same kind of variability can be found in reading biopsy slides, according to Dr. Groopman: There can be significant differences in how different pathologists assess the same biopsy.
Several Examples Presented
From my own personal experience of interactions with patients over the past 21 years, I have shown, in this chapter, multiple examples of the need for and value of getting a second opinion. Space doesn’t permit us to present them all here in the BOB Tales. Here are just a few examples of the importance of a second opinion:
No Bladder Cancer
A couple of years ago a gentleman who was treated with external beam radiation for prostate cancer sent me the following email:
I was treated with radiation for prostate cancer four years ago at the age of 65. Last August, because of blood in my urine I went to my urologist and after testing was recommended for a biopsy.
They diagnosed me with invasive bladder cancer. My urologist said it was aggressive but treatable.
Based on your recommendation, I decided to seek a second opinion from Johns Hopkins. They suggested it may not be cancer but something that mimics it called pseudo-neoplastic legions. Upon learning that I was treated with radiation therapy, it reinforced their conclusions. Johns Hopkins suggested I send my slides to Cedars Sinai and Memorial Sloan Kettering. They were both in agreement with Johns Hopkins. What a relief! I had a follow-up biopsy, and this time there was no evidence of any cancer at all and this was confirmed by Johns Hopkins.
I was encouraged to write to you after reading the December BOB Tales newsletter regarding the importance of getting second opinions. There appears to be a relationship between radiation and inflammation that can occur afterwards that
mimics cancer that most pathologist aren’t aware of.
Thank you, Brotherhood of the Balloon. If it weren’t for your encouragement to get a second opinion, I would have been treated for bladder cancer for no reason at all.
Gleason Score Increased
One gentleman who read the first edition of my book was diagnosed with Gleason 3+4=7 prostate cancer. He decided to follow my suggestion and have his biopsy slides examined by one of the premier labs listed in the appendix.
The results were quite shocking: Gleason 5+5=10! The good news is this individual was properly treated for a much more advanced prostate cancer. In all likelihood, his treatment for Gleason 3+4 cancer would have been much less aggressive, leaving him with a significantly greater chance of a recurrence. Today, several years later, his PSA is 0.4 and he’s enjoying life to the fullest.
Gleason Score Decreased
Here’s an email I received from another patient who followed my advice:
First of all, I want to extend much thanks to you for recommending a second opinion on my biopsy slides. I did so and as a result, my Gleason score was reduced from 3+4=7 to 3+3=6 and my core volume reduced from 15 percent to 5 percent. Per NCCN, using this information, I would be considered in the very low-risk category.
According to NCCN, people in the very low risk category with life expectancy less than 20 years, active surveillance is a very good option. This is what I plan to do after I fire my urologist. To the very end, he refused to send the slides for a second opinion; he told me if I want it that I should do so myself.
No Cancer at All! – Example 1
A gentleman who was diagnosed with prostate cancer was scheduled for a radical prostatectomy. He read my book, got a second opinion, and learned he didn’t have prostate cancer. He was deliriously happy with this good news and posted the following review of my first book on Amazon:
Always get a second opinion on your diagnosis. April 6, 2007
In January of 2007, at the age of 55, I was diagnosed with prostate cancer. My urologist wanted to operate within two weeks. After finding Bob Marckini’s book, “You Can Beat Prostate Cancer and You Don’t Need Surgery to Do It,” I read it from cover to cover and took his advice. I had my slides reviewed by another pathologist. The results conflicted with the original report, so I sent the slides to Dr. Jonathan Epstein at Johns Hopkins, who is recommended in Bob’s book. He stated that I needed another biopsy to be certain, since he could not say that it definitely was cancer. After having the second biopsy... the results came back that I did not have prostate cancer. Had I not read this book I may very well have had needless surgery. This is definitely a “must read” for every man diagnosed with prostate cancer. Don’t leave your life in the hands of one doctor. Always do your homework and make sure it includes this book.
No Cancer at All! – Example 2
Another gentleman who had been diagnosed with prostate cancer was encouraged by his urologist to have DaVinci laparoscopic robotic surgery. The patient did his homework and narrowed his choices to either DaVinci surgery or proton therapy.
He contacted Loma Linda University Cancer Center for information about proton therapy and they sent him a packet of material, which included a copy of my book. He read the book, followed my suggestions on getting a second opinion on his pathology slides, and discovered that he didn’t have prostate cancer! Greatly relieved, he posted a review of my first book on Amazon, which is reproduced in my book.
Finding Out When It Was Too Late
One gentleman who lives in my hometown was diagnosed with prostate cancer. He took his urologist’s advice and had his prostate removed surgically. Following surgery, when his prostate was dissected and examined by a pathologist, no cancer was found!
In all likelihood, a second opinion on his biopsy slides would have shown no cancer, which means the surgery and subsequent life-altering side effects could have been avoided.
Examples like these are rare, but they do happen. Often the second opinion confirms the first reading, but it’s not uncommon for the second opinion to be different from the first, resulting in better information on which to base the best treatment option.
Summary
It’s rare when the second opinion is significantly different from the first, but it’s not rare for one of the premier pathology labs to differ from the initial pathology reading. I have seen many cases where a 3+3 was found to be a 3+4 or a 4+3. I have also seen cases where a 4+4 was found to be a 3+4 or a 3+3.
These differences are critically important and can often mean the difference between choosing a simple treatment for early-stage disease – including active surveillance – or aggressive, invasive, radical therapies for advanced disease.
Bottom line: The reading of pathology slides is subjective at best. It’s common for two pathologists to report different Gleason scores when prostate cancer is diagnosed. It’s important to know the “true” score so your treatment protocol can be properly designed. Under-treating can result in a recurrence, and over-treating could result in damaging quality-of-life issues. It’s always wise to get a second opinion on your biopsy results from a reputable pathology lab.
Important Announcement!
We have an important announcement to make about Bob’s book in our April Newsletter. Stay tuned!
Did you find Bob’s new book helpful?
If you found Bob’s book helpful, please write a review on Amazon.
We’re happy to discount books in quantity (minimum 20) to anyone interested in spreading the word on proton therapy. Just send an email to Deb Hickey. Proceeds from book sales are used to help fund our efforts and to support proton therapy research.
The Kindle version is free to Kindle Unlimited members or can be purchased for $9.99 for non-members. The paperback price is $22.45. Buy You Can Beat Prostate Cancer second edition on Amazon or Lulu Press.

National Proton Conference
 The National Association for Proton Therapy (NAPT) will be holding its next annual conference in St. Petersburg, FL, April 3-6, 2022. There will be two full days of in-person engagement, education, and collaboration among experts in the proton therapy world.
The National Association for Proton Therapy (NAPT) will be holding its next annual conference in St. Petersburg, FL, April 3-6, 2022. There will be two full days of in-person engagement, education, and collaboration among experts in the proton therapy world.
Exhibits: There are typically large halls filled with exhibits showing the latest developments in proton therapy technology, equipment, systems, and support systems. Information is presented on new particle accelerator design, new beam delivery systems, more precise control systems, and many things connected with proton therapy.
Attendance: Proton therapy centers from all over the world send representatives to the conference. Often clinicians and clinical leaders from all the major U.S. proton centers are in attendance, and many participate in panel discussions. Other attendees include physicists, senior administrative officials, and vendors who design and make equipment, products, and systems that support proton therapy and related technologies.
Panels and Presentations: Several presenters and panels will address a variety of proton-related issues ranging from the latest developments in proton therapy research, clinical and technological advances in proton therapy, global proton initiatives, and the economics and sustainability of proton center development and growth.
![]()
![]()

Last Month’s Brain Teaser
How many squares are there?
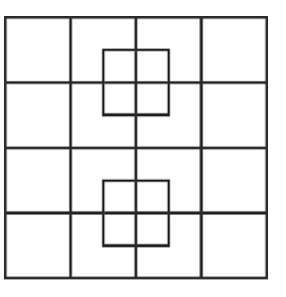
Answer: 40
Here’s a video that provides a detailed explanation.
Winner: We received lots of guesses last month. Many members sent in several guesses. There were only six members who answered correctly! The winner of the signed copy of Bob Marckini’s book is from Owings Mills, MD and wishes to remain anonymous.
![]()
![]()
New Brain Teaser
Here’s a brain teaser for our “lateral thinking” members.
Rearrange the following group of letters to form a single word:
S N E W G A L R D O I
Send your brain teaser answer to [email protected] for a chance to win a signed copy of Bob Marckini’s NEW second edition book, You Can Beat Prostate Cancer.
Hard Landing
We have lots of airline pilots in our group. One of them sent us this story.
An airline pilot wrote that on a recent flight he had hammered his ship into the runway really hard. The airline had a policy that required the first officer to stand at the door while the passengers exited, smile, and give them a “Thanks for flying our airline.”
He said, considering his bad landing, he had a hard time looking passengers in the eye, thinking that someone would have a smart comment.
Finally, everyone had gotten off except for a little old lady walking with a cane. She said, “Sir, do you mind if I ask you a question?”
“Why, no Ma’am,” said the pilot. “What is it?”
The little old lady said, “Did we land, or were we shot down?”
Today’s World
Theme parks can snap a crystal-clear picture of you on a roller coaster going 70 mph, but bank cameras can’t get a clear shot of a robber standing still.
Someone posted that they’d just made synonym buns. I replied, “you mean just like the ones that grammar used to make?” I’m now blocked.
To paranoid people who check behind their shower curtains for murderers: if you find one, what’s your plan?
The more I get to know people, the more I realize why Noah let only animals on the boat.
Facial recognition software can pick a person out of a crowd but the vending machine at work can’t recognize a dollar bill with a bent corner.
COVID-19 Fact: 87 percent of gym members don’t even know their gym is closed.
Some people seem to have aged like fine wine. I aged like milk – I got sour and chunky.
Dear Sneeze: If you’re going to happen, happen. Don’t just put a stupid look on my face and then leave.
We all know Albert Einstein was a genius, but his brother Frank was a monster.
Children Are Quick (Source)
Teacher: Why are you late?
Student: Class started before I got here.
Teacher: Glenn, how do you spell “crocodile?”
Glenn: K-R-O-K-O-D-I-A-L
Teacher: No, that’s wrong
Glenn: Maybe it is wrong, but you asked me how I spell it.
Teacher: Donald, what’s the chemical formula for water?
Donald: H I J K L M N O
Teacher: What are you talking about?
Donald: Yesterday you said it was H to O.
Teacher: Winnie, name one important thing we have today that we didn’t have 10 years ago.
Winnie: Me!
Teacher: Now, Simon, tell me frankly, do you say prayers before eating?
Simon: No sir, I don’t have to, my mum is a good cook.
Teacher: Clyde, your composition on “My Dog” is exactly the same as your brother’s. Did you copy his?
Clyde: No, sir. It’s the same dog.
Teacher: Harold, what do you call a person who keeps talking when people are no longer interested?
Harold: A teacher.
![]()
![]()

Estate Planning Hints
BOB Member Ron Hendricks is Director, US Foundation for Trinity Western University. He regularly copies us on his “News from Ron” mailings, which are helpful hints on estate planning to the readers of his newsletters. We have found Ron’s suggestions to be timely and beneficial. With his permission we periodically share some of his wisdom with our membership. This excerpted segment is called …
A Step List to Estate Planning – The Process Doesn’t Need to be Intimidating
- Write a letter of instruction to your executor to keep on file, which names specific individuals to receive certain personal assets.
- Inventory your assets. Be sure to determine the most tax-effective way to distribute your property.
- Choose your beneficiaries. Reflect on the persons and organizations you wish to benefit. Remember to include God’s Kingdom as one of your beneficiaries.
- Calculate your gross estate. State or federal estate tax may be a concern if your estate exceeds the amount sheltered by the exemptions.
- Consider other estate planning documents. You may need a revocable living trust in addition to a will.
- Plan for medical decisions. Ask your adviser about a health care power of attorney and living will.
- Follow through on your estate planning. Be sure that your assets are transferred into your living trust. Don’t leave your trust empty!
- Store your will, living trust and other estate planning documents and directives in a safe place.
- Retain copies of income tax returns.
- Review your estate plans regularly. The death of a spouse, successor trustee or beneficiary are among many things that impact your estate plans.
- Make an appointment with an attorney. If you don’t know one, ask a relative, friend or co-worker that you trust for a referral.
Boy, Were They Wrong! (Source)
There is not the slightest indication that [nuclear energy] will ever be obtainable. It would mean that the atom would have to be shattered at will. ─ Albert Einstein, 1932.
So many centuries after the creation, it is unlikely that anyone could find hitherto unknown lands of any value. ─ Report of the committee organized in 1486 by King Ferdinand and Queen Isabella of Spain to study Columbus’ plans to find a shorter route to India.
When the Paris Exhibition closes, electric light will close with it and no more be heard of. ─ Erasmus Wilson (1878) Professor at Oxford University
They will never try to steal the phonograph because it has no `commercial value. ─ Thomas Edison (1847-1931)
Radio has no future. ─ Lord Kelvin (1824-1907), British mathematician and physicist, ca. 1897.
Rail travel at high speed is not possible because passengers, unable to breathe, would die of asphyxia. ─ Dr. Dionysus Lardner (1793-1859), Professor of Natural Philosophy and Astronomy at University College, London.
The horse is here to stay, but the automobile is only a novelty—a fad. ─ Advice from a president of the Michigan Savings Bank to Henry Ford’s lawyer Horace Rackham. Rackham ignored the advice and invested $5,000 in Ford stock, selling it later for $12.5 million.
Part II next month …
![]()
![]()
Quote of the Month:
“Expecting the world to treat you fairly because you are a good person is a little like expecting the bull not to attack you because you are a vegetarian.” – Dennis Wholey
![]()
![]()

The Other Side (Source)
A sick man turned to his doctor as he was preparing to leave the examination room and said, “Doctor, I’m afraid to die. Tell me what lies on the other side.”
Very quietly, the doctor said, “I don’t know.”
“You don’t know? You, a religious man, don’t know what’s on the other side?”
The doctor was holding the handle of the door; on the other side came a sound of scratching and whining, and as he opened the door, a dog sprang into the room and leaped on him with an eager show of gladness.
Turning to the patient, the doctor said, “Did you notice my dog? He’s never been in this room before. He didn’t know what was inside. He knew nothing except that his master was here, and when the door opened, he sprang in without fear.”
“I know little of what’s on the other side of death, but I know one thing … I know my Master is there and that’s enough.”
Low PSAs to all,
Bob Marckini and Deb Hickey
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file.
NO MEDICAL ADVICE: Material appearing here represents opinions offered by non-medically-trained laypersons. Comments shown here should NEVER be interpreted as specific medical advice and must be used only as background information when consulting with a qualified medical professional.