Dear Members (a note from Deb Hickey):
The tiny office on our second floor was designed for one. I know this because my desk had to be taken apart and reassembled just to get it through the door. Adding another desk in here was just ridiculous. When my husband is seated at his, the backs of our rolling chairs touch.
Mark – who’s working from home – has no less than 8 video conference calls a day. I gather there are roughly 20 people on each Zoom. They probably judge the back of my head while they quibble (loudly) about website designs and client demands. I wear headphones and make sure my hair is brushed.
I just stopped “homeschooling” my daughter, Gemma, since school officially ended in mid-June. That’s a good thing because I was about to expel her. Getting my daughter to sit still for an hour is like trying to put tights on a fish.
Mark has become quite the cook and he’s been preparing most of the meals. The downside is that when he’s finished, it looks like the kitchen imploded. The countertops are sticky; the stove is draped in semi-solid emulsion; and the grime on the floor needs to be peeled off with a putty knife. Some nights I’d rather just have Fruit Loops.
Camp is closed. That means my daughter will be home for the next two months practicing her science experiments in the bathroom and decorating every room in the house with Lego parts and Barbie clothes. The other day she filled the microwave with gummi bears and set the timer for 15 minutes. Have you heard the saying, “cleaning your house while your kids (or kid plus husband) are home is like brushing your teeth while eating Oreos”?
Being holed up at home, as we’ve all been for the past few months, can be hard. COVID-19 has done much more than grind the most public aspects of our lives to a halt. It’s also disrupted our most meaningful relationships. Togetherness is a good thing usually, but what happens when we’re together too much?
I’ve literally had to sit down and discuss this very question with my husband. During that conversation we realized you can’t spell “divorce” without “COVID,” and we had a little laugh.
But really, communication is best. What we were able to tolerate before, we may now need to talk about. That prevents the annoyance from turning into anger.
Mark and I have also decided to send our daughter to a private school for children with dyslexia. The tuition costs more than my first house. Did I mention Mark got a 30 percent pay cut? Obviously, these things also add to our stress. And that stress exacerbates each of our idiosyncrasies.
So, when his computer keyboard clacking starts to make my jaw clench, it’s a good time to take a break and get outside – even if it’s just to take the dog for a walk. Alone time is important. I also think it’s important to be extra understanding during this time together. If I’m cranky and overly sensitive, I may not be the only one in my house feeling this way.
I remind myself often – this too shall pass. I also try to seek out the good all around me: My husband is always home for dinner; Lucy the doodle is in the best shape of her life because she’s getting about 47 walks a day (This has also stopped her from eating our furniture); Gemma has so much free time to play outside (and work on her fairy house); and we’re saving money on gas and dinners out.
I hope those of you who are still hunkered down at home are hanging in there …
Please note this issue is our two-month summer edition and the next issue will be for September. As always, we have a full and comprehensive newsletter for you. We begin with a detailed update on the COMPPARE trial comparing proton therapy to IMRT for prostate cancer; there are new clinical trial results that show a novel pill for ADT may work better than Lupron injections for men with advanced prostate cancer; there’s a new study that shows proton therapy is associated with a lower risk of secondary cancers than IMRT and 3D conformal radiotherapy; we include frequently asked questions and answers, for cancer patients as they’re treated during the coronavirus pandemic; we report on the recent rise in advanced prostate cancer cases and if PSA screening standards are to blame; and much more.
We hope you enjoy this issue of BOB Tales and, as always, we welcome and encourage your valuable feedback. Please send an email to [email protected].
Deb Hickey
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file.
In This Issue:
- The COMPPARE Trial: A Path to Improve Future Health Outcomes for Men with Prostate Cancer
- Novel Drug for ADT Could be Game Changing
- Proton Therapy Associated with Lower Risk of Secondary Cancers than IMRT and 3D Conformal Radiotherapy
- Cancer Treatment During COVID-19: An FAQ for Patients
- Advanced Prostate Cancer Cases Rising: Are PSA Screening Standards to Blame?
- A Pea May Pack a Mighty Anticancer Punch
- Canned, Cooked Tomatoes Protect Against Prostate Cancer
- Eating Organic Foods can Dramatically Reduce Risk of Cancer
- The Benefit of Adding Coconut Milk to Sweet Potatoes
![]()

The COMPPARE Trial: A Path to Improve Future Health Outcomes for Men with Prostate Cancer
Why is COMPPARE so important?
 Most private insurers won’t cover proton therapy for prostate cancer due to its higher cost and the fact that there’s been no comprehensive clinical comparison between proton therapy and conventional (photon) radiation. Some insurers still refer to proton therapy as “experimental” and/or “investigational” (though it’s been in use for more than 50 years - and was FDA approved for treating cancer more than 30 years ago).
Most private insurers won’t cover proton therapy for prostate cancer due to its higher cost and the fact that there’s been no comprehensive clinical comparison between proton therapy and conventional (photon) radiation. Some insurers still refer to proton therapy as “experimental” and/or “investigational” (though it’s been in use for more than 50 years - and was FDA approved for treating cancer more than 30 years ago).
The COMPPARE clinical trial will directly compare the potential benefits and harms of protons versus photons (IMRT) in treating prostate cancer. It will emphasize patient-centered outcomes (side effects, cure rate, and quality of life) and will help future patients make informed treatment decisions. The results will also provide insurers with the data needed to make coverage and policy decisions around the use of proton therapy for prostate cancer.
The COMPPARE trial is funded by the Patient-Centered Outcomes Research Institute (PCORI) and led by Dr. Nancy Mendenhall, medical director from the University of Florida Health Proton Therapy Institute. Bob Marckini is a member of the COMPPARE executive board, and Deb Hickey serves on the caregivers-stakeholders group.
Enrollment
The COMPPARE trial is enrolling 3,000 patients (1,500 proton and 1,500 IMRT) – men age 30-85 – and will run approximately five years. Patients will answer brief surveys regarding treatment choice, quality of life, and side effects for at least three years. Modest compensation will be provided.
It’s important to note that patients in the COMPPARE trial can choose which treatment option they’d prefer, and they will receive the standard of care.
Some patients in the COMPPARE trial who qualify, may choose to participate in an embedded, randomized controlled trial comparing the standard treatment protocol to a shortened (hypofractionated) treatment protocol.
COMPPARE Trial Goals
The goal is to answer the following patient-centered questions:
- How likely are men to experience different quality of life issues with protons versus photons?
- How likely are men to experience different side effects with either treatment?
- Which treatment will result in a better cure rate?
- Is a shorter treatment regimen as safe and effective as the standard treatment regimen?
Who’s Eligible?
In general, to be eligible for the COMPPARE trial you must be:
- A man diagnosed with non-metastatic prostate cancer;
- A candidate for radiation therapy;
- Between the ages of 30-85 with a life expectancy ≥8 years.
Since our last BOB Tales update on COMPPARE, a decision to expand eligibility criteria was established. The following five changes were implemented:
- The maximum age of participants increased from 80 to 85;
- Life Expectancy Estimation (LEE) was decreased from ≥ 10 years to ≥ 8 years;
- Very low-risk patients are included;
- Patients with prior Benign Prostatic Hyperplasia (BPH) procedures, such as TURP and GreenLight Laser, are included;
- Inflammatory Bowel Disease (IBD) is an exclusion only if a patient is undergoing active treatment or is symptomatic.
A Hurdle
Earlier this year, the COMPPARE team was on track to meet site activation and patient accrual milestones. However, COVID-19 hit in early March and the accrual rate fell rapidly. Some participating centers (sites) halted all research initiatives. Others were allowed to follow patients already enrolled in the trial, but not allowed to enroll new patients. Almost all sites observed a significant decrease in the referral of prostate cancer patients for radiation therapy due to delays in prostate biopsies, as most non-emergency surgery and other treatments were postponed.
In light of these issues, PCORI agreed to negotiate revised accrual milestones at the end of summer. The team is hopeful that clinical and research practices will return to normal by then.
What’s the latest?
As of this writing, 45 sites have been activated nationnwide and patient accrual is at 20 percent (611) of the 3,000 population goal. While all sites are working hard to develop best practices for ensuring safety among patients, COMPPARE trial leaders are collaborating with site participants to accelerate the recruitment process.
Find weekly activation and enrollment updates on the COMPPARE website.
You can help!
If you know anyone who has recently been diagnosed with prostate cancer and considering proton therapy or IMRT, please tell them about the COMPPARE trial. Remember, the patient chooses the treatment he wants and his standard of care will not change unless he chooses to participate in the embedded, randomized hypofractionation trial.
Potential candidates are welcome to visit the participant information page on the COMPPARE website and/or email [email protected] with questions about the trial.
Novel Drug for ADT Could be Game Changing
Clinical trial results show a new hormone therapy pill – relugolix – works better than standard injections for men with advanced prostate cancer. The drug has the “potential to become a new standard for ADT and advanced prostate cancer,” said Neal D. Shore, MD, medical director for the Carolina Urologic Research Center, Myrtle Beach, SC.
Relugolix also cut the risk of heart attack or stroke by 54 percent as compared to standard ADT therapy, leuprolide (Lupron).
This could be an important advantage, Shore noted. “The percentage of patients with prostate cancer dying of cardiovascular disease has surpassed the percentage of patients dying from prostate cancer itself since the early 1990s,” he said. “Approximately 30 percent of men with prostate cancer have known cardiovascular disease, and many more of these patients have comorbid risk factors including obesity, diabetes, hypertension, and hyperlipidemia.”
Relugolix isn’t approved by the FDA, though it’s approved in Japan for use in the treatment of uterine fibroids, but at a much lower dose. Shore suggests that if it becomes FDA approved, it will be “game-changing.”
Proton Therapy Associated with Lower Risk of Secondary Cancers than IMRT and 3D Conformal Radiotherapy
In a recent study, researchers from Standford Medicine used data from the National Cancer Database, which captures 70 percent of all U.S. cancer patients on a registry. They identified nine million cancer patients – pediatric and adult – who were treated for a first cancer diagnosis between 2004 and 2015. Among those identified, 450,373 received 3D conformal radiation, IMRT, or proton therapy for non-metastatic cancer. Tumor types included head and neck, gastrointestinal, gynecologic, lymphoma, lung, prostate, breast, bone/soft tissue, and brain/central nervous system.
Of the 450,373 patients, 33 percent had 3D, 65 percent had IMRT, and just 1.3 percent had proton therapy. Median follow-up was 5.1 years. Investigators compared the incidence of second malignancy among patients. Surprisingly, the data showed no difference in second cancers between 3D and IMRT patients. Another significant finding was the incidence of second cancer with proton therapy was less than a third the rate of second malignancies with either 3D or IMRT. In fact, the second malignancy odds ratio which was 1 for both 3D and IMRT, was only 0.31 with proton therapy – a significantly lower rate. This reduced rate of second malignancy with proton was consistent across all groups – pediatric, middle-aged, senior, male, and female patients.
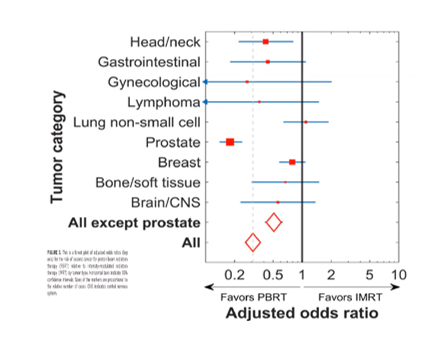 In the graph to the left, the red square represents the rate of second malignancy. If there’s a reduced rate of second malignancy with IMRT, the red square appears on the right side of the vertical black line. If there’s a lower rate of second malignancy with proton therapy, the red square appears on the left side of the black line.
In the graph to the left, the red square represents the rate of second malignancy. If there’s a reduced rate of second malignancy with IMRT, the red square appears on the right side of the vertical black line. If there’s a lower rate of second malignancy with proton therapy, the red square appears on the left side of the black line.
If the horizontal blue line crosses the center black line, it means the finding may not be statistically significant. As you can see, with two sites – head and neck at the top and prostate in middle – the blue line does not cross the central line. That means there is a significantly lower rate of second malignancy with proton therapy in head and neck and prostate cancer patients.
The diamond on the bottom of the graph represents all patients in the study. As you can see, the odds ratio is about 0.3 which shows a significantly lower rate of second malignancy with proton therapy in the overall population of patients.
Interestingly, researchers decided to exclude prostate cancer, which is represented by the diamond above the bottom diamond. It’s also significant that when the prostate cancer patients are excluded, there’s a significantly lower rate of second malignancy (.5) – about half as many cancers after proton therapy.
Finally, you’ll notice the only site where the red square ends up to the right of the black line is lung cancer. This could be because those patients may have a poor survival rate and might not be living long enough for a second malignancy.
 Cancer Treatment During COVID-19: An FAQ for Patients
Cancer Treatment During COVID-19: An FAQ for Patients
As of this writing, the U.S. has the greatest number of positive coronavirus cases in the world. As a result, proton therapy centers and radiation oncology clinics are working hard to protect patients from COVID-19 while continuing to run effective treatment programs. As physicians and staff adapt to a reduction in referrals and develop new safety strategies, what can cancer patients expect when they go in for proton therapy, IMRT or SBRT? The COMPPARE clinical trial team, led by Dr. Nancy Mendenhall, compiled some frequently asked questions to help answer your questions. Some of them are below.
What should I do to prepare for my appointment?
- Make sure you understand all telemedicine options available to you. Some on-treatment visits and follow-up visits will be conducted over the phone, unless your case requires a physical examination.
- Please call your doctor before you come for your treatment if you have:
- A fever, cough, or shortness of breath;
- Had exposure to someone with a positive COVID-19 diagnosis;
- Traveled outside of the U.S. in the past 14 days;
- Traveled on a cruise ship in the past 14 days.
- Plan on minimizing the amount of supplies you bring to your appointment.
What if I’m traveling from out of state?
- Your treatment facility will most likely contact you well in advance of your appointment to help you understand their approach to patient scheduling.
- Some facilities require out-of-state patients self-quarantine before their arrival (i.e. 14 days of self-quarantine prior to visit, simulation, or initiation of therapy, and a continuation of self-quarantine while under treatment).
- Some facilities require new out-of-state patients to have a negative test result for COVID-19 prior to proceeding with their first appointment.
Who can come with me to my appointment?
- Some facilities allow one caretaker per patient during consult appointments only. Others have established zero-visitor policies, with exceptions for adults with neurocognitive impairments and for pediatric patients.
- Caretakers, other than for pediatric patients, are sometimes asked to remain outside for all other appointments.
- Often, no children under the age of 12 or 18 are allowed, unless they are the patient.
What can I expect when I arrive?
- Often, patients are asked to arrive no more than 10 minutes before their scheduled appointment time.
- Many institutions have established separate patient and employee screening checkpoints at main entrances.
- When you arrive at your institution, you and your caretaker will most likely be screened before you enter the building.
Advanced Prostate Cancer Cases Rising: Are PSA Screening Standards to Blame?
According to a new study by researchers from the American Cancer Society, cases of advanced prostate cancer in the U.S. are rising while early stage prostate cancer diagnoses are declining. The reason is likely due to the changes in screening guidelines over the past two decades.
What were they thinking?!
We first notified our readers in 2011 that a report had been issued by the U.S. Preventive Service Task Force (USPSTF) recommending against PSA testing because they said, “there is a moderate or high certainty that the PSA test has no net benefit or that the harms outweigh the benefits.”
Here’s a recap from our October 2011 issue of BOB Tales:
Fundamentally, the USPSTF is recommending the PSA test be abolished. They seem to base their recommendation on the fact that prostate cancer is usually slow growing, and that many, if not most, men would probably not experience severe pain or death from the disease. This may be true, but what about those men who would experience severe pain and/or death from prostate cancer? Should they be ignored?
The USPSTF believes that the consequences from treatment can be significant, including impotence, incontinence, and even death. However, they appear to be looking at the consequences of treating with surgery, and the resulting quality-of-life issues, when making this determination. If someone is diagnosed with what we refer to as “early stage, garden-variety prostate cancer,” which is slow growing and unlikely to produce symptoms, it makes no sense to surgically remove the prostate when the risk of impotence, incontinence, and other morbidity is so high. In this case, it may be true that, “the harms outweigh the benefits.” But does it not make sense to treat with a painless, non-invasive modality (proton therapy) that would likely destroy the cancer and not impact quality of life?
Certainly there are cases where some prostate cancers have been treated when active surveillance may have been a better alternative. But to broad-brush the issue and recommend the termination of PSA testing is absurd in our opinion.
 Here are the facts: Tens of thousands of men are cancer free today because they were tested; the cancer was found early; and their treatment worked. Many of these would have suffered and eventually died from the disease if they hadn’t been treated.
Here are the facts: Tens of thousands of men are cancer free today because they were tested; the cancer was found early; and their treatment worked. Many of these would have suffered and eventually died from the disease if they hadn’t been treated.
Before PSA testing, physicians wouldn’t treat the disease until it presented symptoms, such as problems with urine flow, blood in the urine, loss of weight, pain in the lower back or pelvis, or a lump in the prostate. The problem is that by the time these symptoms show up, the disease may be advanced and the patient’s options limited.
We believe the problem is not over-diagnosing, it’s over-treating and the widespread use of invasive treatments that often leave the patient with debilitating side effects.
Dr Gary Kirsh, president of The Urology Group, agrees there’s some merit to the USPSTF’s decision-making as PSA testing may diagnose early stage cases of the disease, potentially prompting unnecessary treatments and biopsies. However, “the problem with that kind of thinking, while it has some validity, is that it did not recognize doctors’ ability to change and understand the use of the test over time,” Kirsh said. “So what happened was that the USPSTF threw the baby out with the bathwater. Years later, the chickens have come home to roost, and we’re beginning to document a shift in the number of diseases presenting in a noncurable state.”
Early Detection Still Critical
While overdiagnosis has been a concern for the USPSTF panel, experts say PSA testing is still critical in detecting early cases of prostate cancer. “It’s a test that has to be used with wisdom, and the wisdom is that everyone with an elevated PSA doesn’t need to be biopsied, and, more important, everyone with a small amount of early, nonaggressive prostate cancer doesn’t need to be treated,” explained Kirsh.
Steven Eisenberg, DO, a Calfiornia oncologist specializing in prostate cancer, feels there should be a measured approach to bridge the gap between overtreatment and potentially missing a diagnonsis. This would involve a “powerful partnership” between patients and doctors – one with open dialogue, thoughtful communication, and an individualized approach for each patient.

Attention: Members with Hip Replacements
We occasionally ask our members to volunteer to be included on a former proton patient reference list. These categorized lists (by location, treatment protocol, existing health condition(s), etc.) are emailed to newly diagnosed men when they contact us in the midst of the treatment decision-making process and would like to connect with others who’ve been in their shoes. They’re typically interested in your experience of treatment, any side effects you endured, and how you’re doing after treatment.
We tell all newly diagnosed men who contact us that speaking with former patients – at least 10 representing each treatment option they’re considering – is the best way to get honest and accurate information.
We’ve received an overwhelming response from members in the past when we’ve asked for volunteers. We’re hoping for the same response this time.
If you’ve had a hip replacement, single or bilateral, before you underwent proton treatment, please let us know if you’d agree to be listed on our hip replacement patient reference list. Men who’ve had hip replacements are typically concerned that the proton beam passes through the hips and would be blocked by metal. Some doctors have told them they can’t
have any form of radiation therapy for this reason. Of course we know this isn’t true as we have dozens and dozens of members who’ve had hip replacments before they were treated with protons. The treatment plan must be customized because the beam can’t pass through
the metal hips. Not all proton centers treat men with single or bilateral hip replacements,
but some do.
Please email Deb Hickey and let us know if you’d be willing to receive emails and/or phone calls from men with hip replacements who are considering proton therapy for their prostate cancer. We expect you to receive only a handful of emails/phone calls a year.

We’ve been producing BOB Tales newsletters monthly for almost 20 years. During this time there have been articles that many new members haven’t seen, and some older members may have forgotten. So, we periodically re-run some articles from past newsletters. This one from November 2005 is titled:
A Pea May Pack a Mighty Anticancer Punch
Pack your pantry with bean, pea, and lentil soups to warm you up all season long. According to RealAge.com, peas, lentils, and beans contain a compound that may help protect you against cancer. The compound, inositol pentakisphosphate, inhibits a key pathway in cancer cell growth. The discovery may one day lead to new cancer-fighting treatments. A diet rich in inositol pentakisphosphate, a compound found in legumes, nuts, and wheat bran, may help protect you against cancer by interfering with the fine network of blood vessels tumors need to develop.
Round out your diet with plenty of cancer-fighting foods, such as snow peas, sugar snap peas, black beans, broccoli, tomatoes, citrus fruits, soy, and calcium-rich, low-fat dairy. Limit red meat consumption to no more than one serving per week; high intake has been linked to an increased risk of certain types of cancer.
![]()

You Can Beat Prostate Cancer:
And You Don’t Need Surgery to Do It – Second Edition
Bob Marckini’s new book has been out for only three months and it’s already climbed to the No. 1 position on an Amazon search for books on “prostate cancer.” The old book is still in the top 10 – in the No. 7 position. What delights us the most, is that for the first time ever, the book is ahead of the prostate cancer surgery “guru’s” book, Dr. Patrick Walsh’s Guide to
Surviving Prostate cancer.” Bob studied an earlier edition of this book when he was diagnosed 20 years ago. To many, it is considered “the bible” for prostate cancer patients. But not to us. We think there’s a new book that should have that distinction.
A physician who read Bob’s book wrote a heartfelt, comprehensive and compelling review on Amazon recently. Here are some excerpts:

Having prostate cancer can scare the daylights out of anyone – even a physician like me. I’ll never forget how bad I felt when those shocking words,“You have an advanced and aggressive cancer,” were spoken by a urologist who’d just met me and didn’t know me enough to really care. I was terrified and devastated and needed help. Most of all, I wanted a confident reassurance that I was going to survive and, better yet, become cancer free. That someone turned out to be Bob Marckini and his heroic book, You Can Beat Prostate Cancer. The first edition was great; the new edition is outstanding; and I’ll tell you why.
First, you can trust everything written in this book. Even before you finish reading it, you’ll know as I did, a physician for 45 years, that its contents are true and reliable. You can literally bet your life on it. As a leading medical university professor, I did just that.
With this book in your hands, you’ll no longer feel helpless or hopeless. Why? Because it’ll be impossible for you to single handedly attempt to find, read, study, and comprehend the vast medical knowledge about prostate cancer. Bob’s done it for you. He’s distilled the many scientifically intricate and advanced ways to successfully treat prostate cancer into an easy-to-read and well-referenced guidebook. You shouldn’t try to beat prostate cancer without this book as your trusted resource and companion. This book is loaded with all the essential and extremely useful information about prostate cancer. It’s easy to read and understand.
… I also found the book riveting and couldn’t and wouldn’t put it down. With each page I felt more hope returning. And long before I was done, I felt as though my cancer had already been cured, at least in my mind, because I discovered and selected the treatment that was going to be the best for me. And I knew from Bob’s book the outstanding results that others had achieved with my exact cancer.
I’m just getting started with my treatment and my wife and I have every reason to smile with relief. For now, I’m in good hands and about to receive what Bob’s book, and my doctors have assured me is the absolute best choice of treatment …
Thank you, Bob, for this miracle book. I hope it ends up in the hands of everyone who has prostate cancer and their loved ones … I hope it’s read by those men who don’t even know when to begin taking steps for prostate examination and PSA testing. For that is the best way to assure the earliest detection and receive the best and most appropriate treatment to be cancer free. But mostly, I hope this book takes away that dreadful looming fear of having cancer and instills a promising belief that you can be the next one, amongst a brotherhood of many, who have beaten cancer, thanks to Bob and this book.
What a great review! You can probably guess which treatment he chose.
Reminders
The second edition of You Can Beat Prostate Cancer includes a complete update on prostate cancer prevention, imaging technology, diagnostic technology, treatment options, and virtually all aspects of the latest developments in proton therapy.
Proton centers are beginning to acquire the new book and send it to patients making inquiries about proton therapy. We have no doubt this will educate patients on the benefits of proton therapy and help them with their treatment decisions.
We are happy to discount books in quantity (minimum 20) to anyone who is interested spreading the word on proton therapy. Just send an email to [email protected]. Proceeds from book sales are used to help fund our efforts and to support proton therapy research.
Please note: The Kindle version is free to Kindle Unlimited members or can be purchased for only $9.99, for non-members. The soft-cover price is $22.45

Buy You Can Beat Prostate Cancer second edition on Amazon or Lulu Press.
![]()

Canned, Cooked Tomatoes Protect Against Prostate Cancer
 A recent study by Loma Linda University Health shows cooked tomatoes may reduce the risk of prostate cancer. Researchers found that men who consumed canned and cooked tomatoes five to six times per week had a 28 percent decreased risk of the disease compared with men who never consumed the fruit.
A recent study by Loma Linda University Health shows cooked tomatoes may reduce the risk of prostate cancer. Researchers found that men who consumed canned and cooked tomatoes five to six times per week had a 28 percent decreased risk of the disease compared with men who never consumed the fruit.
Lead author, Gary Fraser, MBChB, PhD, said the effect was significant even after adjusting for several potential confounders including ethnicity, weight, physical activity levels, and others. “Interestingly, the decreased risk was seen only in those men who ate canned and cooked tomatoes,” Fraser said. There was no significant association between prostate cancer and consumption of raw tomatoes, tomato soup, tomato sauce and tomato-based vegetable juice.
Eating Organic Foods Can Dramatically Reduce Risk of Cancer
A groundbreaking study published in the Journal of the American Medical Association found that eating organic foods – those grown without artificial chemicals, hormones, antibiotics, or genetically modified organisms (GMOs) – can dramatically reduce your risk of developing cancer.
French scientists tracked the diets of nearly 69,000 adults over four-plus years. They found those who consumed the most organic foods were 25 percent less likely to develop cancer – especially lymphomas and post-menopausal breast cancer – than those who rarely or never ate organic foods.
This is one of many studies that have found links between organic foods and improved health.
The Benefit of Adding Coconut Milk to Sweet Potatoes
Longevity expert Dan Buettner, founder of the Blue Zones and New York Times-bestselling author of The Blue Zones: Lessons for Living Longer from the People Who’ve Lived the Longest, suggests “upgrading” your potatoes from classic ruddy-skinned russetts to sweet. Sweet potatoes are rich in vitamins, minerals, antioxidants, and fiber. According to Buettner, they’re also the cornerstone of the diet of the world’s longest-living people. To boost their health benefit, Buettner suggests pairing sweet potatoes with coconut milk. The milk lowers the potato’s glycemic load and the sugars absorb more slowly which makes it less likely to appear on your hips and more available to use as energy.

National Proton Virtual Conference
The eighth annual National Proton Conference, which was scheduled for April 26-29, 2020 in Nashville, TN, was canceled due to the coronavirus outbreak. After evaluating options, the team at the National Association for Proton Therapy (NAPT) has decided to provide a one-day virtual conference on Friday, July 24, 2020.
The all-day virtual event is designed to ensure attendees don’t miss out on access to the premier educational event for the proton therapy community. The robust agenda and interactive capability will make this conference a valuable opportunity to access the latest information and resources in the proton world.
Highlights
- Opening Remarks with Olympic Gold Medalist Scott Hamilton
- 40+ Industry Speakers and Presenters
- Hot Clinical Topics in Proton Therapy
- The Future of Particle Therapy
- Innovation Hall with the Opportunity to Live Chat with Industry Experts
- Educational Sessions Focused on Advocacy and Business Development
- Prize Giveaways and NAPT 30th Anniversary Toast with Live Music from Grammy-Nominated Jazz Musician Nicole Zuraitis

Thank You
The BOB mission is three-fold:
- To support each other before, during, and after treatment;
- To promote proton therapy worldwide, and;
- To give something back, with emphasis on supporting proton therapy research.
You – our members – have responded generously to our repeated requests to give back over the past 20 years. Every month we see a list of contributions from members—big and small – from members recently treated and those treated 10, 15 and even 20-plus years ago. We are grateful. Every gift sends us a message that you’re listening to us, and that you care about the future of proton therapy and the many lives that will be spared and the quality of lives that will be maintained – men, women, and most important, children.
We’re proud that the Robert J. Marckini Endowed Chair is funded at $3+ million and supports important research at LLUCC. Nearly half of our members have contributed a total of more than $12 million to various programs at Loma Linda University Health, including members who were treated at proton centers other than LLUCC. Collectively, we’re making a huge difference.
Give to Proton Therapy Research
- Donate online.
- Write a check to LLUCC Proton (Put “Marckini Chair” on the memo line) and mail to LLUH, Office of Philanthropy P.O. Box 2000, Loma Linda, CA 92354.
- Call Regina Joseph at 909-558-5010.

Travel Scam: Public USB Charging Stations for Phones, Computers, and iPads
The March/April issue of SaturdayEveningPost.com reported on a growing scam. Many of the ubiquitous USB free charging stations in airports, hotel lobbies, and other public places have been discovered to contain malware. They can secretly double as a data port that, in a process commonly called “juice jacking,” covertly downloads your data. They can also allow access to your device to someone located nearby. It’s recommended that you carry your own power source to prevent this type of data theft. Plugging your charger into a public AC outlet should also be a way around data theft.
Why and Because
Why do men’s clothes have buttons on the right while women’s clothes have buttons on the left?
Because when buttons were invented, they were expensive and worn primarily by the rich. Since most people are right-handed, it’s easier to push buttons on the right through holes on the left. Because wealthy women were dressed by maids, dressmakers put the buttons on the maid’s right! And that’s where women’s buttons have remained.
Why are zero scores in tennis called “love”?
Because in France, where tennis became popular, the round zero on the scoreboard looked like an egg and was called “l’oeuf,” which is French for “the egg.” When tennis was introduced in the U.S., Americans (naturally), mispronounced it “love.”
Why is shifting responsibility to someone else called “passing the buck”?
Because in card games, it was once customary to pass an item, called a buck, from player to player to indicate whose turn it was to deal. If a player didn’t wish to assume the responsibility of dealing, he’d pass the buck to the next player.
Why is someone who’s feeling great “on cloud nine?”
Because types of clouds are numbered according to the altitudes they attain, with nine being the highest cloud. If someone is said to be on cloud nine, that person is floating well above worldly cares.
Why are many coin collection jar banks shaped like pigs?
Because long ago, dishes and cookware in Europe were made of dense orange clay called “pygg.” When people saved coins in jars made of this clay, the jars became known as “pygg banks.” When an English potter misunderstood the word, he made a container that resembled a pig and it caught on.

Last Month’s Brain Teaser
How can you take 2 from 5 and leave 4?
Answer: The number 5 is spelled F I V E. If you remove two letters – the F and the E, it leaves IV (Hey – we didn’t say it was going to be fair … or even logical).
Winner: BOB member Howie O’Brien of Hansville, WA is last month’s brain teaser winner. Congratulations, Howie! Your signed copy of Bob Marckini’s new book is in the mail.
New Brain Teaser
Three men are walking across a green and luscious field. Only two of them are wearing rubber boots and yet the feet of the third man remain dry. Why? (Think hard.)
Send your answer to [email protected] for a chance to win a signed copy of Bob Marckini’s NEW second edition book, You Can Beat Prostate Cancer.
COVID-19 Humor
The coronavirus pandemic has left many of us feeling frightened and unsure about the future. However, laughter is good for us – and one of the main coping mechanisms during periods of unease – so we hope you’ll enjoy the following jokes.
New monthly budget: Gas $0, Entertainment $0, Clothes $0, Groceries $2,799
Breaking News: Wearing a mask inside your home is highly recommended. Not so much to stop COVI D-19, but to stop eating.
When this quarantine is over, let’s not tell some people.
Not to brag, but I haven’t been late to anything in over eight weeks.
People keep asking: “Is coronavirus really all that serious?” Listen folks, the churches and casinos are closed. When heaven and hell agree on the same thing, it’s probably serious.
Never in a million years could I have imagined I’d go up to a bank teller wearing a mask and ask for money.
For the second part of this quarantine do we have to stay with the same family, or will they relocate us? Just asking.
My husband purchased a world map and then gave me a dart and said, “Throw this and wherever it lands – that’s where I’ll take you when this pandemic ends.” Turns out, we’re spending two weeks behind the fridge.
BREAKING: The World Health Organization has announced that dogs can’t contract COVID-19. Dogs previously held in quarantine can be released. To be clear, WHO let the dogs out.
Read more COVID-19 humor here and here.
The Innocence of Youth
A little girl was talking to her teacher about whales. The teacher said it’s physically impossible for a whale to swallow a human because even though it’s a very large mammal, its throat is very small.
The little girl stated that Jonah was swallowed by a whale.
Irritated, the teacher reiterated that a whale couldn’t swallow a human; it was physically impossible.
The little girl said, “When I get to heaven, I’ll ask Jonah.”
The teacher asked, “What if Jonah went to hell?”
The little girl replied, “Then you ask him.”
A kindergarten teacher was observing her classroom of children while they were drawing. She walked over to one little girl who was working diligently and asked what the drawing was.
The girl replied, “I’m drawing God.”
The teacher paused and said, “But no one knows what God looks like.”
Without missing a beat or looking up from her drawing, the girl replied, “They will in a minute.”
A Sunday school teacher was discussing the Ten Commandments with her 5 and 6-year-olds. After explaining the commandment to Honor thy Father and thy Mother, she asked, “Is there a commandment that teaches us how to treat our brothers and sisters?”
From the back, one little boy answered, “Thou shall not kill.”
One day a little girl was sitting watching her mother do the dishes at the kitchen sink. She noticed her mother had several strands of white hair sticking out in contrast on her brunette head. She looked at her mother and inquisitively asked, “Why are some of your hairs white, Mummy?”
Her mother replied, “Well, every time you do something wrong and make me cry or unhappy, one of my hairs turns white.”
The little girl thought about this revelation for a while and then said, “Mummy, how come ALL of grandma’s hairs are white?”
The children had all been photographed and the teacher was trying to persuade them each to buy a copy of the group picture. “Just think how nice it will be to look at it when you’re all grown up and say, ‘There’s Jennifer; she’s a lawyer,’ or ‘That’s Michael; he’s a doctor.’”
A small voice at the back of the room rang out, “And there’s the teacher; she’s dead.”
At Sunday school, there was a basket of apples with a written note that said, “Don’t take more than one – God is watching!”
Farther away, there was a box of chocolates. A clever little child wrote a note, “Take as many as you want – God is watching the apples.”
![]()
Quote of the Month: "I hate it when I see a real old person and then realize that we went to high school together."
—Unkown
![]()

With all the hardships we’re enduring with the COVID-19 pandemic, it might be a good idea to look at it from a different perspective:
Imagine You Were Born in 1900 …
On your 14th birthday, World War I starts, and it ends on your 18th birthday. Twenty-two million people perish in that war. Later in the year, a Spanish Flu epidemic hits the planet and runs until your 20th birthday; 50 million people die from it in those two years. Yes, 50 million.
On your 29th birthday, the Great Depression begins. Unemployment hits 25 percent and the World GDP drops 27 percent. That runs until you’re 33. The country nearly collapses along with the world economy.
When you turn 39, World War II starts. You aren’t even over the hill yet. And don’t try to catch your breath because on your 41st birthday, the U.S. is fully pulled into WWII. Between your 39th and 45th birthday, 75 million people perish in the war.
Smallpox is an epidemic until you’re in your 40’s, as it kills 300 million people during your lifetime.
At 50, the Korean War starts. Five million perish. From your birth until age 55, you deal with the fear of polio epidemics each summer. You experience friends and family contracting polio and being paralyzed and/or dying.
At 55, the Vietnam War begins and doesn’t end for 20 years. Four million people perish in that conflict. During the Cold War, you live each day with the fear of nuclear annihilation. On your 62nd birthday you have the Cuban Missile Crisis, a tipping point in the Cold War. Life on our planet, as we know it, almost ends. When you turn 75, the Vietnam War finally ends.
Think of everyone on the planet born in 1900. How did they endure all of that? When you were a kid in 1985, you didn’t think your 85-year-old grandparent understood how hard school was … and how mean that kid in your class was. Yet they survived everything listed above.
Perspective is an amazing art – refined and enlightening as time goes on. Let’s try to keep things in perspective. Your parents and/or grandparents were called to endure all the above – you are called to stay home and sit on your couch.
Low PSAs to all, and have a great – and safe – summer,
Bob Marckini and Deb Hickey
To print the BOB Tales newsletter or view the newsletter with a larger font size, click here for the PDF file.
NO MEDICAL ADVICE: Material appearing here represents opinions offered by non-medically-trained laypersons. Comments shown here should NEVER be interpreted as specific medical advice and must be used only as background information when consulting with a qualified medical professional.